The following resources are available to support with Asthma management.
Accessing CDRC resources on SystmOne
To access the below resources you will need to be a member of the DCS group on SystmOne. To do this, please follow the instructions on the CDRC SystmOne Access webpage.
Asthma Quality Improvement Reports
A series of reports are available to help improve asthma care and identify high risk patients.
These reports are in the folder CDRC Quality > Respiratory
They are also described in a Reports tab on the Asthma CDRC template.
| Report Name | Returns |
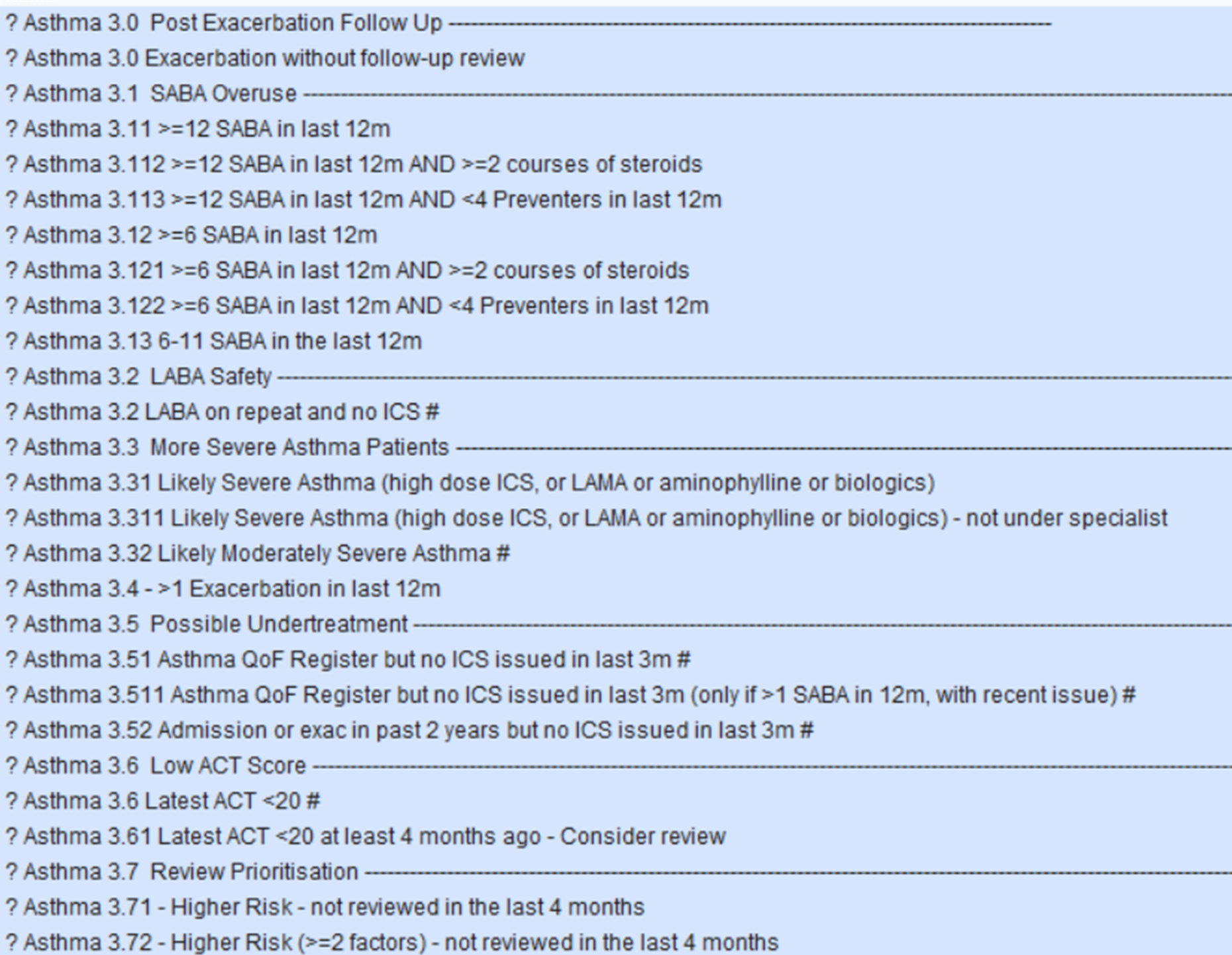
| ? Asthma 3.0 Post Exacerbation Follow Up | —————————————————————————————– |
| ? Asthma 3.0 Exacerbation without follow-up review | Patients who have had an exacerbation in the last year without a subsequent follow-up review |
| ? Asthma 3.1 SABA Overuse | —————————————————————————————– |
| ? Asthma 3.11 >=12 SABA in last 12m | Asthma patients (excluding COPD) receiving treatment that have been issued 12 SABAs in the last 12 months. |
| ? Asthma 3.112 >=12 SABA in last 12m AND >=2 courses of steroids | Asthma patients (excluding COPD) receiving treatment that have been issued 12 SABAs AND equal to, or more than, 2 courses of steroids in the last 12 months. |
| ? Asthma 3.113 >=12 SABA in last 12m AND <4 Preventers in last 12m | Asthma patients (excluding COPD) receiving treatment that have been issued 12 SABAs AND less than 4 ICS in the last 12 months. |
| ? Asthma 3.12 >=6 SABA in last 12m | Asthma patients (excluding COPD) receiving treatment that have been issued 6 SABAs in the last 12 months. |
| ? Asthma 3.121 >=6 SABA in last 12m AND >=2 courses of steroids | Asthma patients (excluding COPD) receiving treatment that have been issued 6 SABAs AND equal to, or more than, 2 courses of steroids in the last 12 months. |
| ? Asthma 3.122 >=6 SABA in last 12m AND <4 Preventers in last 12m | Asthma patients (excluding COPD) receiving treatment that have been issued 6 SABAs AND less than 4 ICS in the last 12 months. |
| ? Asthma 3.2 LABA Safety | —————————————————————————————– |
| ? Asthma 3.2 LABA on repeat and no ICS | Asthma patients with LABAs on repeat but no ICS. |
| ? Asthma 3.3 More Severe Asthma Patients | —————————————————————————————- |
| ? Asthma 3.31 Likely Severe Asthma (high dose ICS, or LAMA or aminophylline or biologics) | Asthma patients that are likely to have severe asthma as they one of the following medications on repeat; a high dose ICS, theophylline/ aminophylline, LAMA, respiratory immunotherapy. |
| ? Asthma 3.311 Likely Severe Asthma (high dose ICS, or LAMA or aminophylline or biologics) – not under specialist | Asthma patients with one of the following medications on repeat; a high dose ICS, theophylline/ aminophylline, LAMA, respiratory immunotherapy – ARE NOT under the care of a respiratory specialist or community team. |
| ? Asthma 3.32 Likely Moderately Severe Asthma | Asthma patients with possible high dose ICS on repeat. |
| ? Asthma 3.4 >1 Exacerbation in last 12m | Patients which have had at least 1 exacerbation in the last 12 months. |
| ? Asthma 3.5 Possible Undertreatment | —————————————————————————————– |
| ? Asthma 3.51 Asthma QoF Register but no ICS issued in last 3m | Patients on the Asthma QoF register that have not had an ICS issued in the last 3 months. |
| ? Asthma 3.511 Asthma QoF Register but no ICS issued in last 3m (only if >1 SABA in 12m, with recent issue) | Patients on the Asthma QoF register that have not had an ICS issued in the last 3 months. Have had at least one SABA issued in last 12 months AND a SABA issued in the last 4 months. |
| ? Asthma 3.52 Admission or exac in past 2 years but no ICS issued in last 3m | |
| ? Asthma 3.6 Low ACT Score | —————————————————————————————– |
| ? Asthma 3.6 Latest ACT Score <20 | Patients whose asthma does not appear to be controlled. |
| ? Asthma 3.61 Latest ACT <20 at least 4 months ago – Consider review | Patients whose asthma did not appear to be controlled at least three months ago and who haven’t subsequently reported an improvement. These patients could be followed up or asked to repeat the ACT test in person or online. |
| ? Asthma 3.7 Review Prioritisation | —————————————————————————————– |
| ? Asthma 3.71 Higher Risk – not reviewed in last 4 months | Asthma patients with indicators of poor control who haven’t been reviewed in the last 4 months. |
| ? Asthma 3.72 Higher Risk – (>=2 factors) – not reviewed in the last 4 months | As Above – increased level of risk. |
| ? Asthma 3.73 Higher Risk – (>=3 factors) – not reviewed in the last 4 months | As Above -increased level of risk. |
| ? Asthma 3.74 Higher Risk – (>=4 factors) – not reviewed in the last 4 months | As Above -increased level of risk. |
Additional reports to help improve care of all Respiratory Diseases
The following reports below are located in the folder CDRC Quality > Respiratory



These reports could be added to a batch reporting process so the relevant person or team in the practice is notified of the results at regular intervals for an ongoing quality improvement process – Automated Reporting
Asthma CDRC Template
How to Access
In the lower left hand corner use the search bar, type in ‘Asthma CDRC’ and select the following template:

Alternatively, press F12 and search for ‘Asthma CDRC’, this will return the aforementioned template.
The Asthma CDRC Template can be used during consultations to provide an overview of current asthma issues, recording of key information, creating/ updating the patient’s personal action plan and more. Expand each node below to view information on each page of the Asthma CDRC template.
The main Asthma page provides an overview of current asthma issues. It is set out in three columns: a column to record important information or link to other templates; a column to show important information and warnings; a column to show expanded information from the record. The asthma page should be completed after the core data template where smoking, weight etc., is covered. The items in a red background are required for QoF.
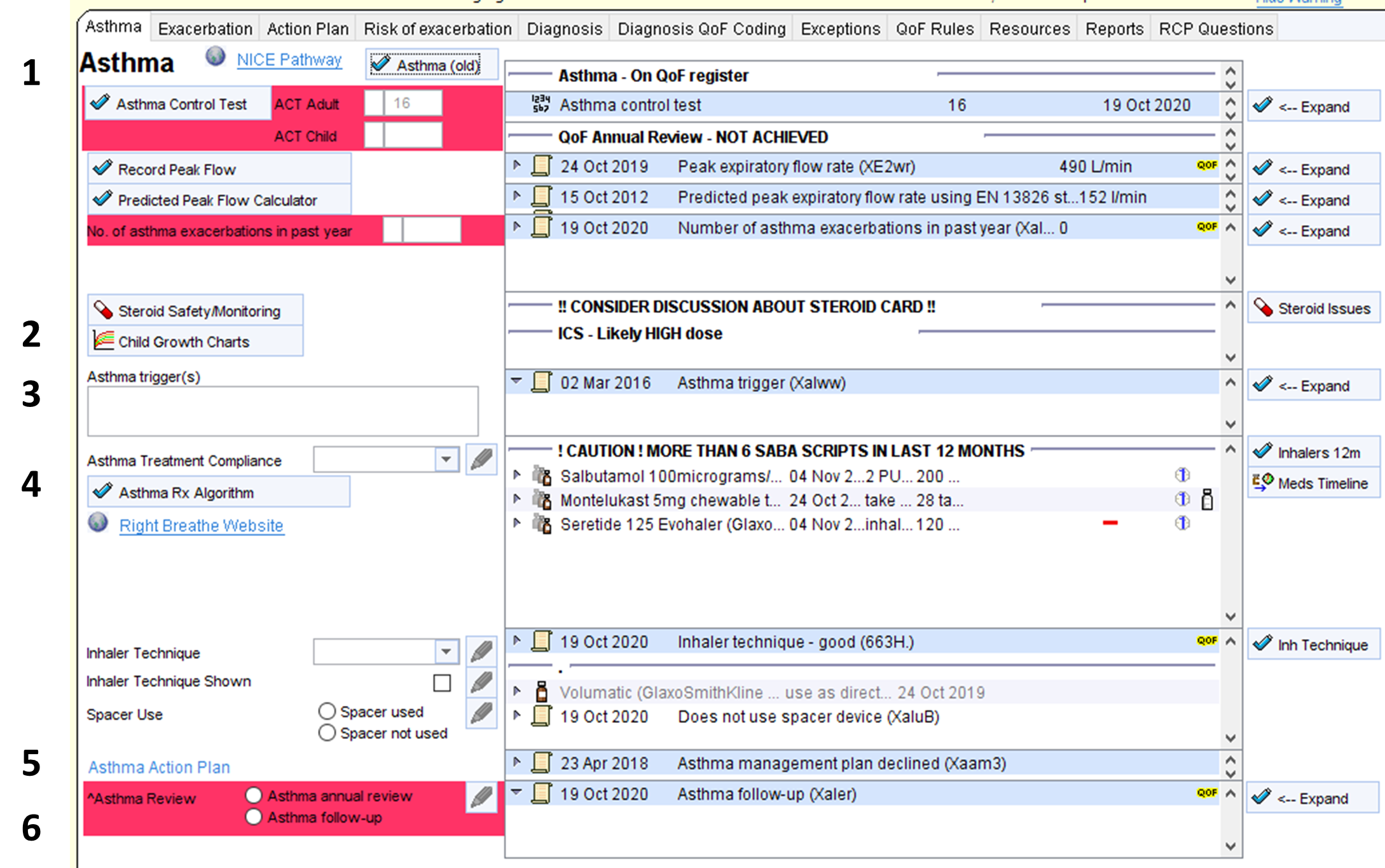
- Current Symptoms
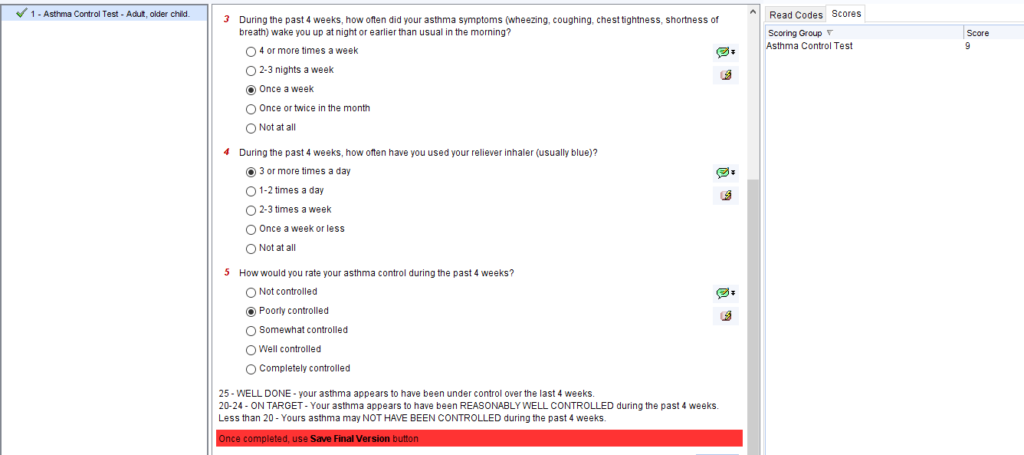
The Asthma Control Test (ACT) protocol takes you through the relevant questionnaire to calculate the ACT score. The child version of the ACT will be selected for children aged 11 and under.
Once completed, click the Save Final Version button above the questionnaire. The ACT score and associated symptoms codes will be recorded automatically. The ACT score will then show on the main template.
If needed, the ACT score can be manually recorded (e.g. if the patient has completed a paper ACT questionnaire) in the boxes on the template
The ACT questionnaire can be completed by the patient in SystmOnline ahead of the asthma review.
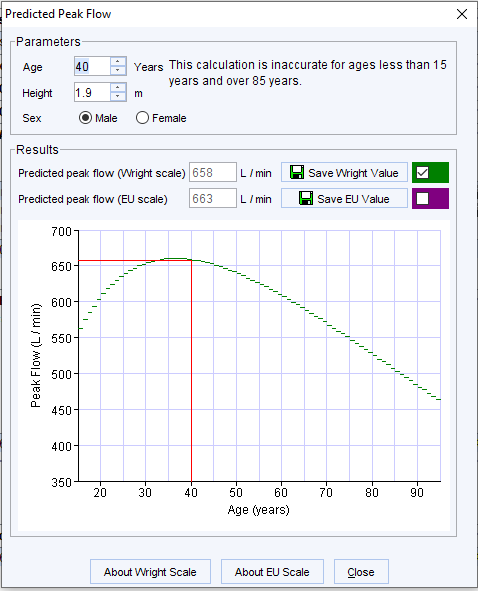
The Peak Flow templates allows recording and interpretation of peak flow readings. A link to child PEFR tables will be shown for children.
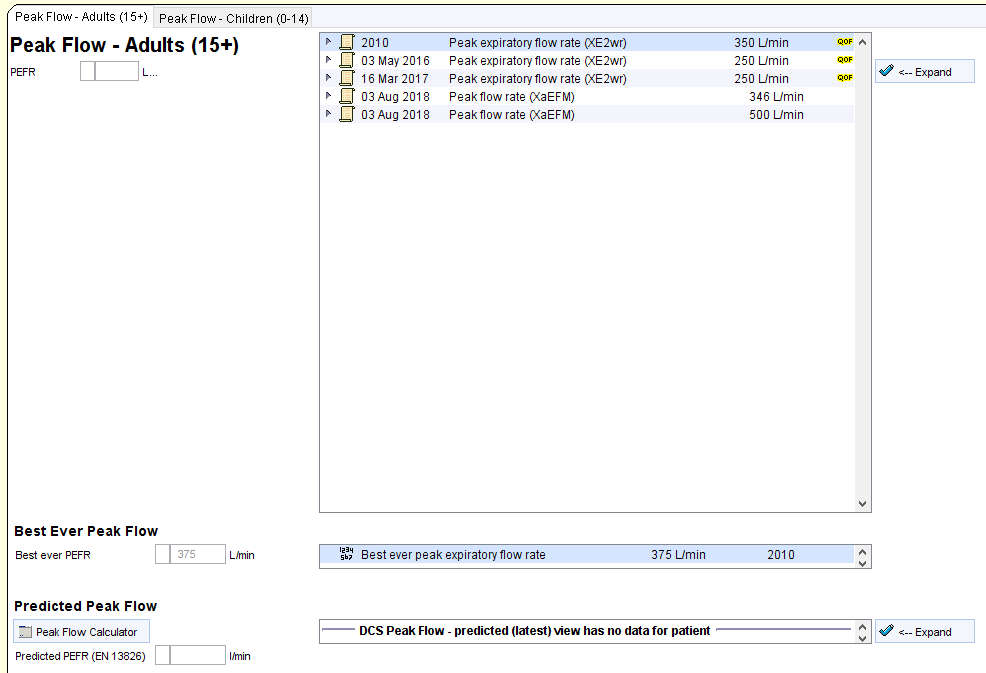
The number of exacerbations is also recorded here – this is a QoF requirement for annual review
The following information is shown in the middle column
- Asthma status (i.e. never had asthma, suspected asthma, previous asthma, current asthma, on asthma QoF register)
- Latest asthma control test score and date
- Whether or not QoF requirement for annual review in the current year is completed, not achieved or excepted
- Latest PEFR
- Latest predicted PEFR
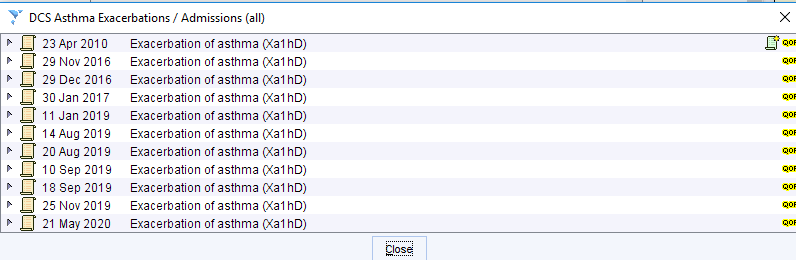
- Information about exacerbations
- Latest record of no’ of exacerbations in the last year
- Warnings showing for patients with
- 2 exacerbations in the last 12m
- Any exacerbation in the last 24m
- Any record of a severe exacerbation
- Any record of hospital asthma admission.
The buttons in the third column will show more detailed information in the same categories
- Steroid Safety
The steroid safety section helps to promote safe use of oral and inhaled corticosteroids.
The steroid safety button links to a steroid monitoring template which helps to give an overview of use of corticosteroids over time, along with safety and monitoring information (NB: template used across multiple clinical areas, not just Asthma):
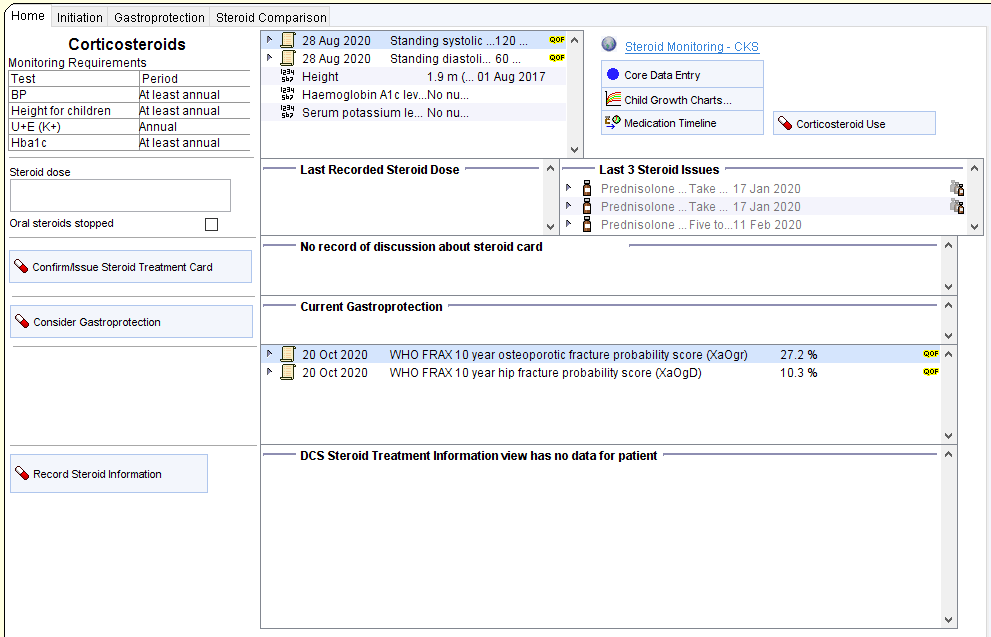
There is a link to the child growth charts for children taking moderate or high dose ICS
The middle column shows the following information:
- Oral steroid issues in the past 12 months
- A warning for patients appearing to be taking high dose ICS
- A warning to consider discussion about steroid safety cards for relevant patients
- A warning when appropriate monitoring is overdue for patients taking oral steroids
The buttons in the third column show expanded information.
- Asthma Triggers
Current asthma triggers can be recorded here. The middle column shows the latest recorded trigger and the button in the third colum shows all previous triggers.
- Asthma Treatment
Compliance with asthma treatment is recorded here
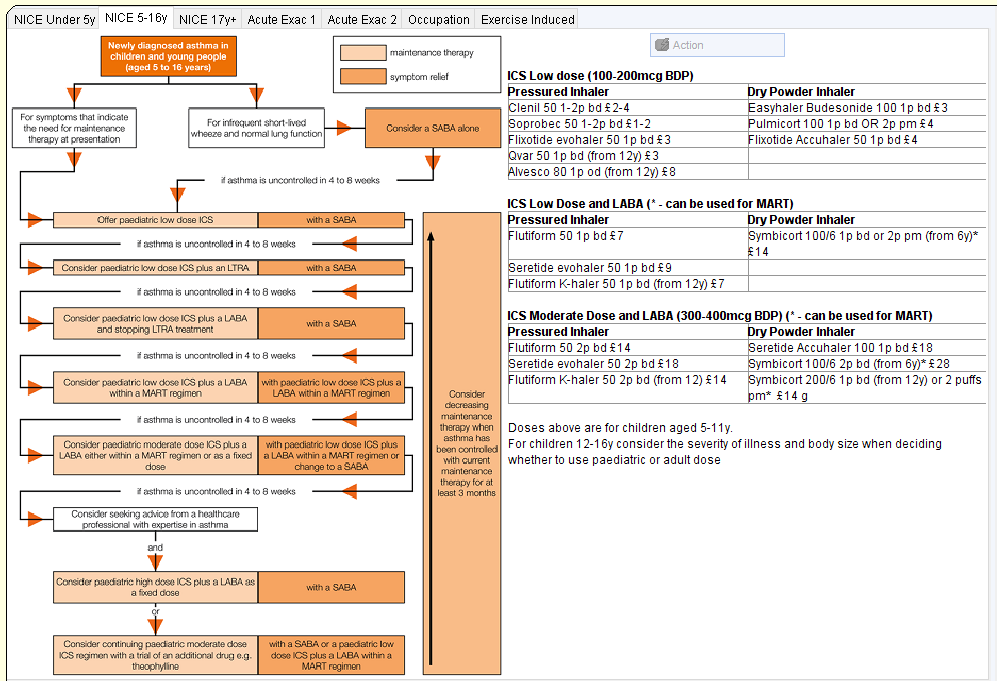
The Asthma Rx Algorithm button links to an overview of up-to-date guidelines to help inform management. The correct tab will be selected automatically based on the patients age.
There is a link to the RightBreathe website which has extensive information about inhalers, spacers, pathways and really useful videos of inhaler techniques for all devices.
Inhaler technique, demonstration of inhaler technique and spacer use can be recorded here.
The middle column will show:
- Latest recorded compliance
- Current asthma medication (including any repeat oral steroids, azithromycin)
- A alert to show if the patient has rhinitis
- The following warnings:
- Patients receiving excessive SABA issues
- Patients with an exacerbation in the past 24m who are not receiving ICS
- Patients who appear to be overusing preventers
- Patients with an apparently unlicensed inhaler
- Patients with inappropriate generic repeats
- Patients who appear to have low concordance for non-ICS preventers
- Latest record of inhaler technique and demonstration
- Latest information about spacer use
- An alert to suggest spacer issue if the patient is on a preventer that is compatible with a spacer which has not been issued in the past 18 months.
The buttons in the third column show more detailed information about medication issues
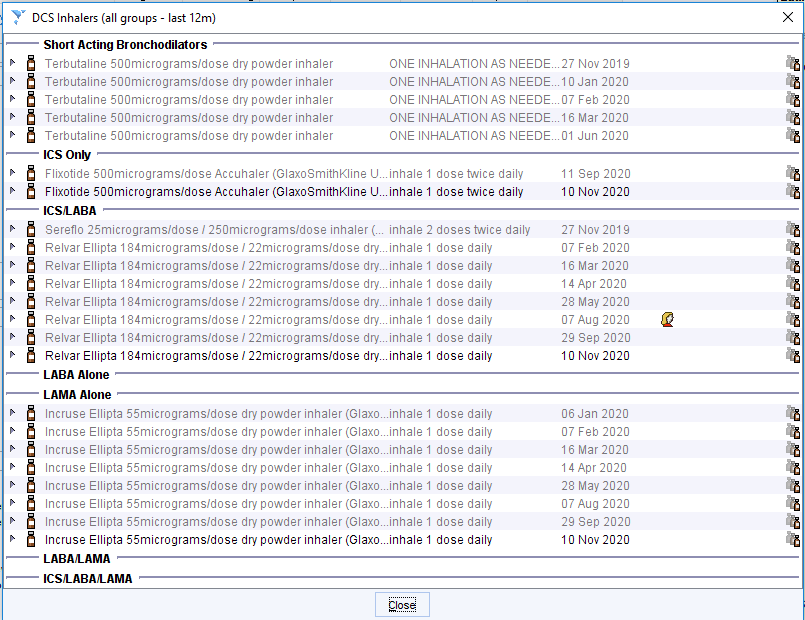
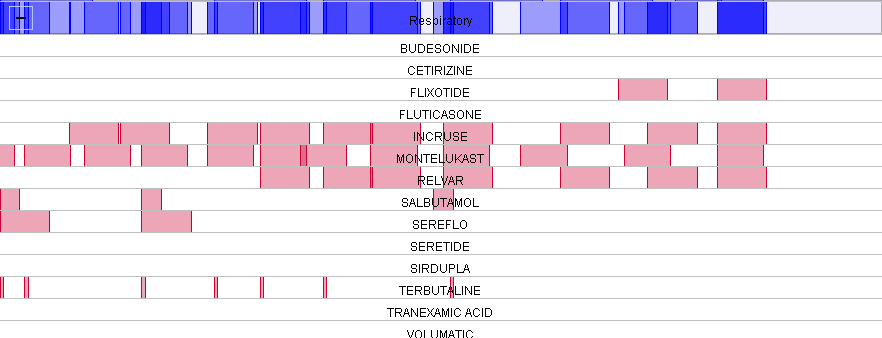
The medication timeline function helps highlight medication concordance and what has been tried before:
- Asthma Treatment Plan
The Asthma Action Plan link goes to the asthma care planning tab of the template
The middle column shows the most recent information about asthma management plans
- Asthma Review
The code for asthma review is recorded here. Details of the main points of the conversation can be recorded as associated text.
The middle column shows the latest asthma review code (and associated text).
The button in the third column shows all previous asthma reviews.
When closing the asthma template, users will be invited to code an asthma review if this hasn’t been done. This is to help improve QoF performance.
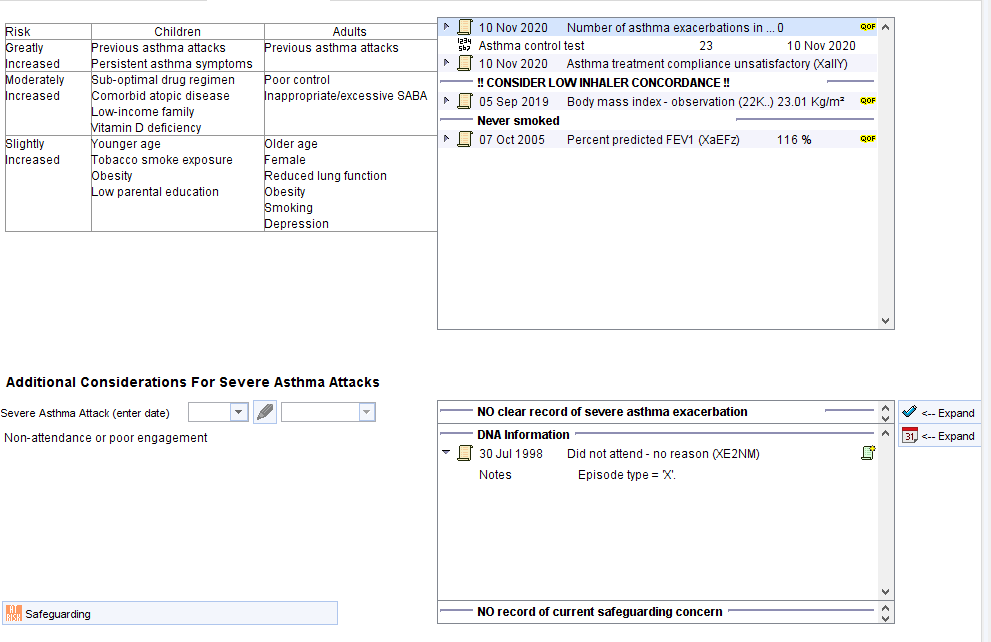
The Exacerbation page of the Asthma CDRC template allows recording of key information required during assessment.
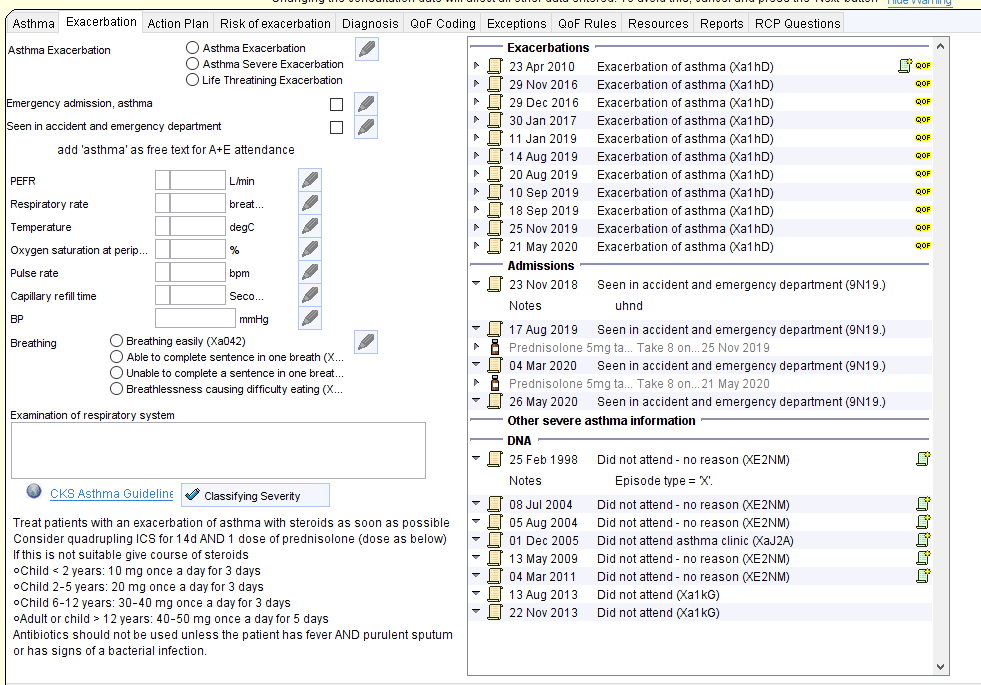
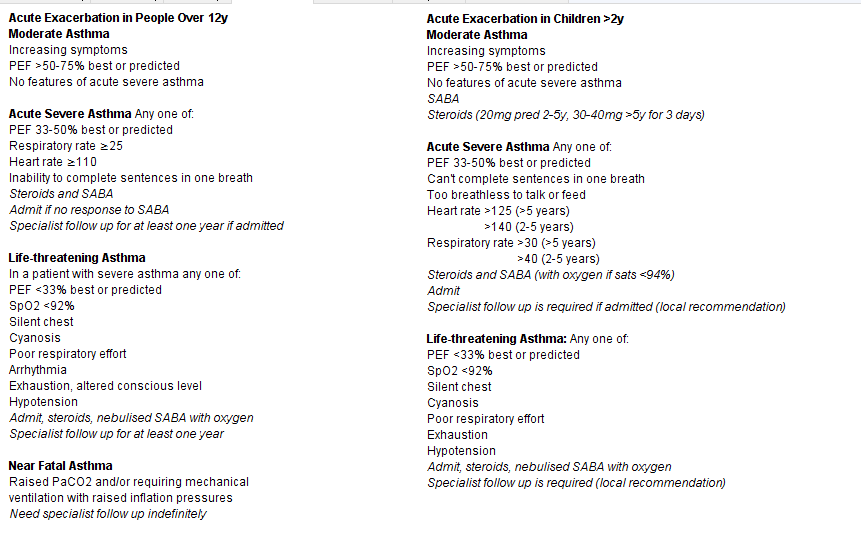
There are links to the CKS page on the management of exacerbations and a quick reference page showing key features for classifying and managing acute asthma.
The right hand column of the template shows information that might be helpful such as: previous exacerbations; previous hospital assessments and admissions; previous steroids; information about previous severe asthma; information about engagement
The Action Plan page allows the viewing, creation and updating of a personal asthma plan.
![Asthma Action Plan
Record Peak Flow
Record Sest Ever Peak Flow
Predicted Peak Flow Calculator
PEFR 80/50/30% sand calculator
Complete Adut Action Plan
Complete Child Action Plan
Complete Seat Action Plan
Create Action Plan
26 Jun 2021 Peak expiratory flow rate
Best ever peak expiratory flow rate
400 LJmin
450 LJmin
12 Jun 2020
26 Jun 2021
Predicted peak expiratory flow rate using EN 13826 limin
Expected peak flow rate x 80%
Expected peak flow rate x 50%
Expected peak flow rate x 30%
Asthma UK Child Asthma Action Plan
320 limin
200 limin
120 limin
12 Jun 2020
12 dun 2020
12 Jun 2020
12 Jun 2020 06 28
Entered by
Finished by
FORBES, Gareth (Dr) (General Medical Practitioner)
FORBES, Gareth (Dr) (General Medical Practitioner) [12 Jun 2020 06:28]
Expand
Expand
All Plans
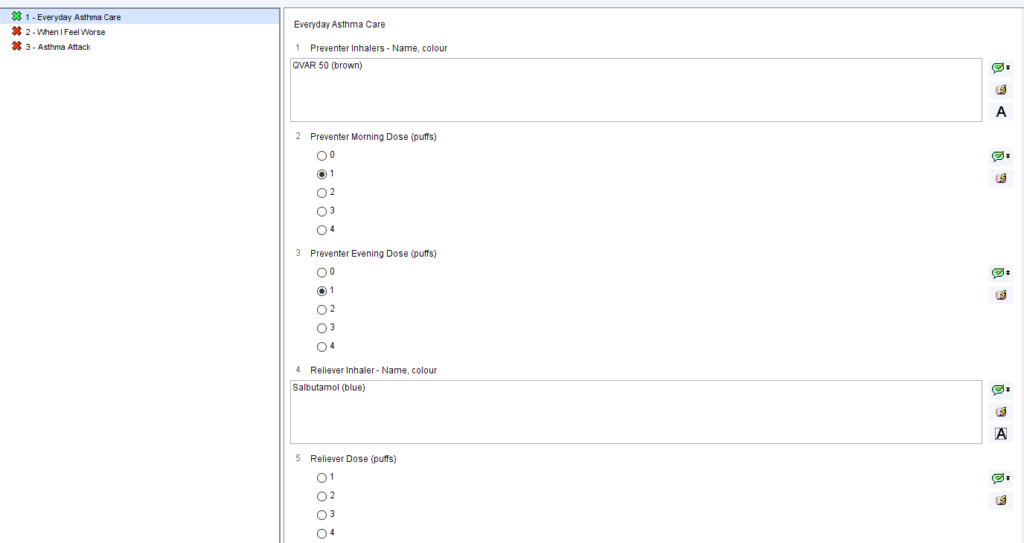
Everyday Asthma Care
Preventer- Name
Preventer- Colour
Preventer Morning Dose (puffs)
Preventer Evening Dose (puffs)
Other daily medicines
Reliever Inhaler- Name
Reliever Colour
Reliever Dose (puffs)
When I Feel Worse
Reliever Inhaler dose (puffs)
Other things to do
Pulmicorl 100
White
montelukast
Salbutamol
Blue
panic
Action Plan
C) Agreed
o
Reviewed
26 Jun 2021
26 dun 2021
9
26 Jun 2021
Asthma Action Plan to Mr Nic-Donotuse Mestpatientkamb
Asthma self-management plan agreed
Patient has a written asthma personal action plan
Action Plan Declined](https://cdrc.nhs.uk/wp-content/uploads/2022/11/image-66.png)
To Create An Asthma Care Plan
If the relevant PEFR results have not already been recorded (they will be shown in the second column), use the buttons to record them. The care plans can be based on either predicted or best ever PEFR.
Click the PEFR 80/50/30% Band Calculator button. Select predicted or best ever PEFR as the baseline at the next screen. The 80/50/30% bands will be recorded and displayed in the second column. (This step is not needed for the BEAT Asthma care plan).
Click on the appropriate Complete ***** Action Plan button. The adult and child plans use the Asthma UK plans. The BEAT plan is for children using the BEATAsthma care plan. Complete the action plan questionnaire. NB clicking the buttons marked ‘A’ will display common presets to make data entry quicker. Once the information is complete, click Save Final Version.
If you wish to amend an existing plan, right click on the box in the second column showing the current plan and choose the Copy Questionnaire option, then choose Copy Comments. An editable version of the previous questionnaire will then be displayed. Amend any entries as appropriate, then click Save Final Version.
Once the questionnaire is complete, click the Create Action Plan button to create a Word care plan, that can be saved and/or printed/emailed to the patient. This button will prompt you to add the relevant QoF asthma plan code. The latest care plan will be displayed in the bottom panel (the entry with the patient’s name) and can be emailed to the patient by right clicking on the entry and choosing Send via NHSMail
Use the final tickboxes on this tab to record that the patient has a care plan.
This page shows the key factors that increase the risk of asthma exacerbation and the relevant information from that patient’s record.
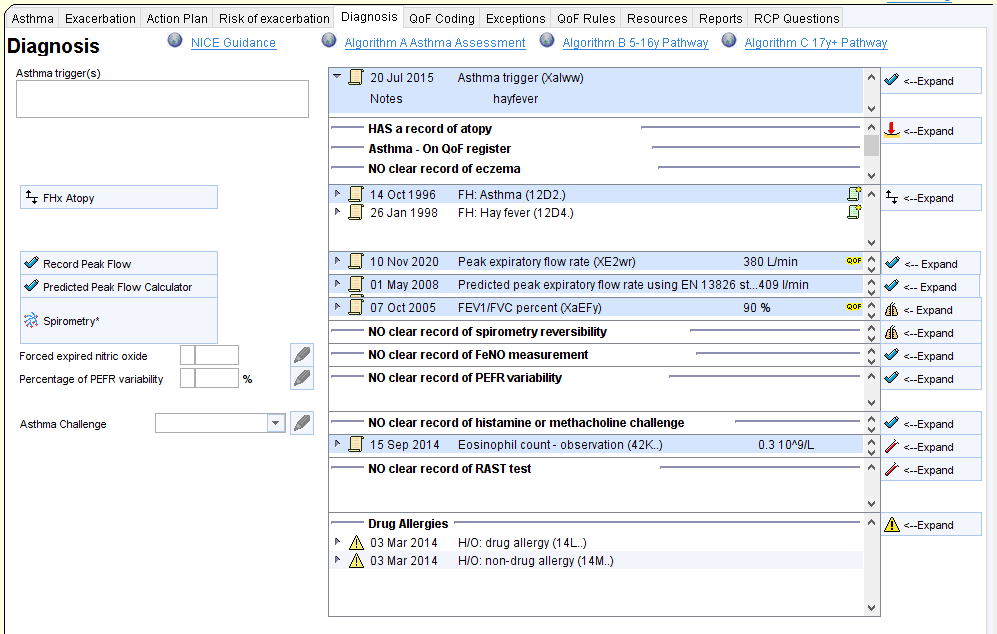
This tab shows the key information required to diagnose asthma. This includes: possible triggers, personal and FHx of atopy, allergy and anaphylaxis; spirometry; FeNO; PEFR variability; asthma challenge results.
The top of the template has links to the NICE assessment algorithms.
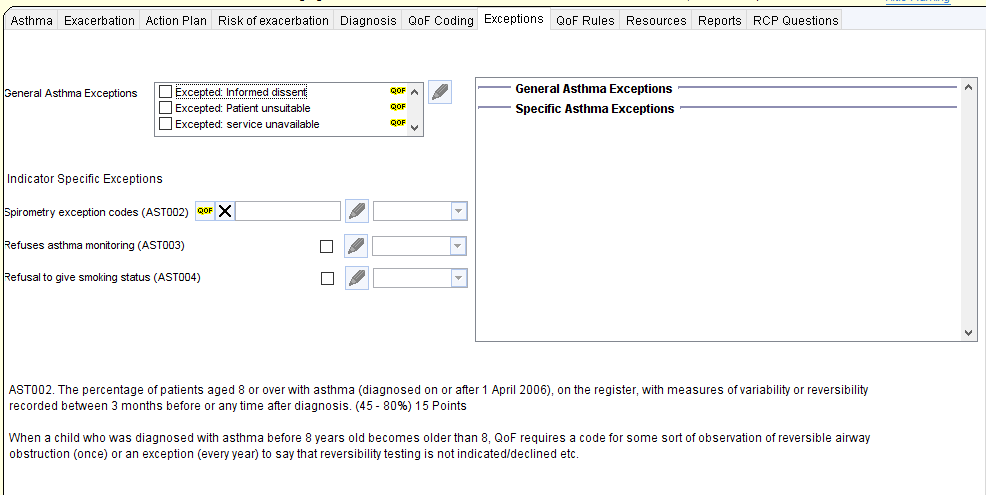
The exceptions page allows recording and viewing of asthma exceptions
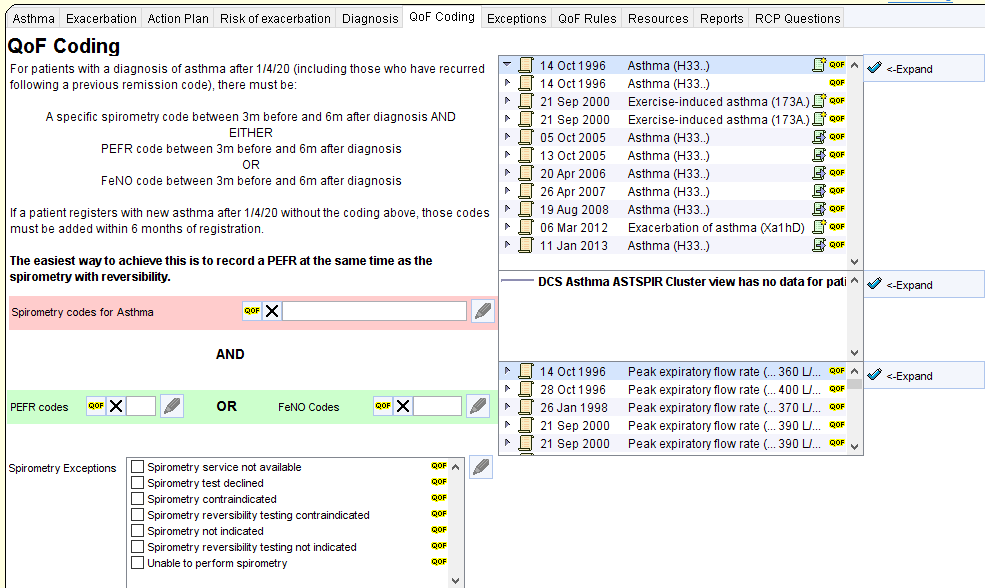
The QoF rules surrounding coding requirements for asthma diagnosis are complex and the business rules do not appear to reflect the QoF specification.
Links to important resources are shown on this tab. Customised local information can be shown on this tab.
Opt-in Resources
The coding requirements for asthma are increasingly complex (and at times nonsensical). The following resources will help keep on top of this. As they are a little intrusive, these protocols need to be enabled at individual practices or CCGs. Contact contact-cdrc@ahsn-nenc.org.uk to enable them
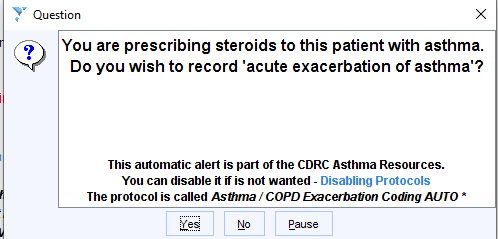
Improve coding of asthma exacerbations
This protocol will trigger for patients with asthma who are prescribed oral steroids if they have not had a code for exacerbation of asthma recorded during the same consultation.
If the patient has COPD and asthma you will be offered the option of coding exacerbation of asthma or COPD or both.
Whenever exacerbation of asthma is coded a prompt will be displayed to advice the user to arrange a follow up within a few days.
Warning if a new diagnosis of asthma is recorded and the QoF business rules for recording spirometry, peak flow and FeNO have not been satisfied.
The following report will identify patients with a relevant new diagnosis without appropriate diagnostic tests. You may wish to add this to an Automated Reporting process.
CDRC Quality > Respiratory > ? Asthma QoF 1.0 – Diagnostic Tests Missing