This page will support you with the Impact and Investment Fund (IIF) 2023 / 2024.
Click here for the Impact and Investment Fund 2023 / 24 Document
Accessing CDRC resources on SystmOne
To access the below resources you will need to be a member of the DCS group on SystmOne. To do this, please follow the instructions on the CDRC SystmOne Access webpage.
Prevention and Tackling Health Inequalities
Vaccination and Immunisation
Percentage of patients aged 18 to 64 years and in a clinical at-risk group who received a seasonal influenza vaccination between 1 September 2023 and 31 March 2024.
Payment range 72-90%
Payment size also determined by number of people at risk.
Use the Influenza Vaccination system to target patients for vaccination
Performance and work to do searches are found in the CDRC Contracting > PCN DES folder:

Patients in the ‘! IIF VI-02 – 18-64y – Influenza vaccine – Work to do (including invited but not vaccinated’ search are those people who have been invited twice but not yet vaccinated. They will not appear in the denominator for the indicator until they are vaccinated.
Percentage of patients aged two or three years on 31 August 2023 who received a seasonal influenza vaccination between 1 September 2023 and 31 March 2024.
Payment Range: 64-82%
Payment also depends on number of patients aged 2-3y on 1st September, without an exception
Use the Influenza Vaccination system to target patients for vaccination
Performance and work to do searches are found in the CDRC Contracting > PCN DES folder:
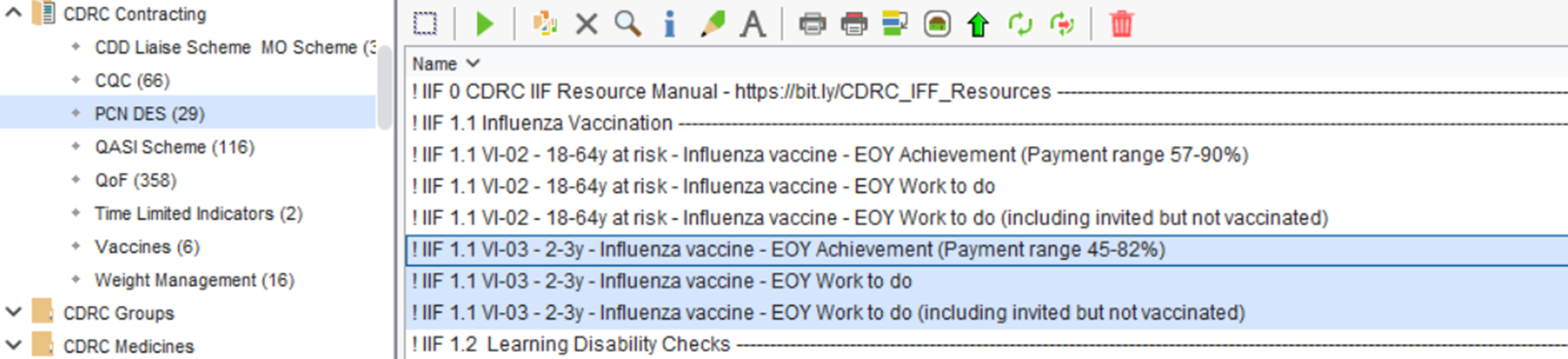
Patients in the ‘! IIF VI-03 – 2-3y – Influenza vaccine – Work to do (including invited but not vaccinated’ search are those people who have been invited twice but not yet vaccinated. They will not appear in the denominator for the indicator until they are vaccinated.
Tackling Health Inequalities
Percentage of patients on the QOF Learning Disability register aged 14 or over, who received an annual Learning Disability Health Check and have a completed Health Action Plan in addition to a recording of ethnicity.
Payment range 60-80%
Payment also depends on number of patients with LD.
Use the Learning Disabilities system to complete the review and care plan.
Performance and work to do searches are found in the CDRC Contracting > PCN DES folder:
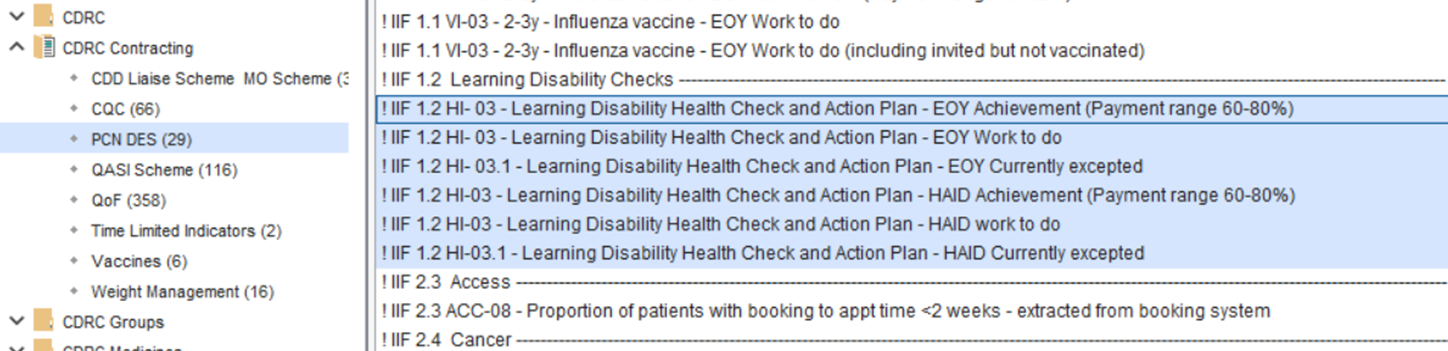
Tips to Achieve This Indicator
Patients in the ‘! IIF 1.2 HI- 03.1 – Learning Disability Health Check and Action Plan – EOY / HAID Currently Excepted’ searches are those people who have been exception reported in the current year. They would add to performance and payment if review and health check were completed.
Providing High Quality Care
Cancer
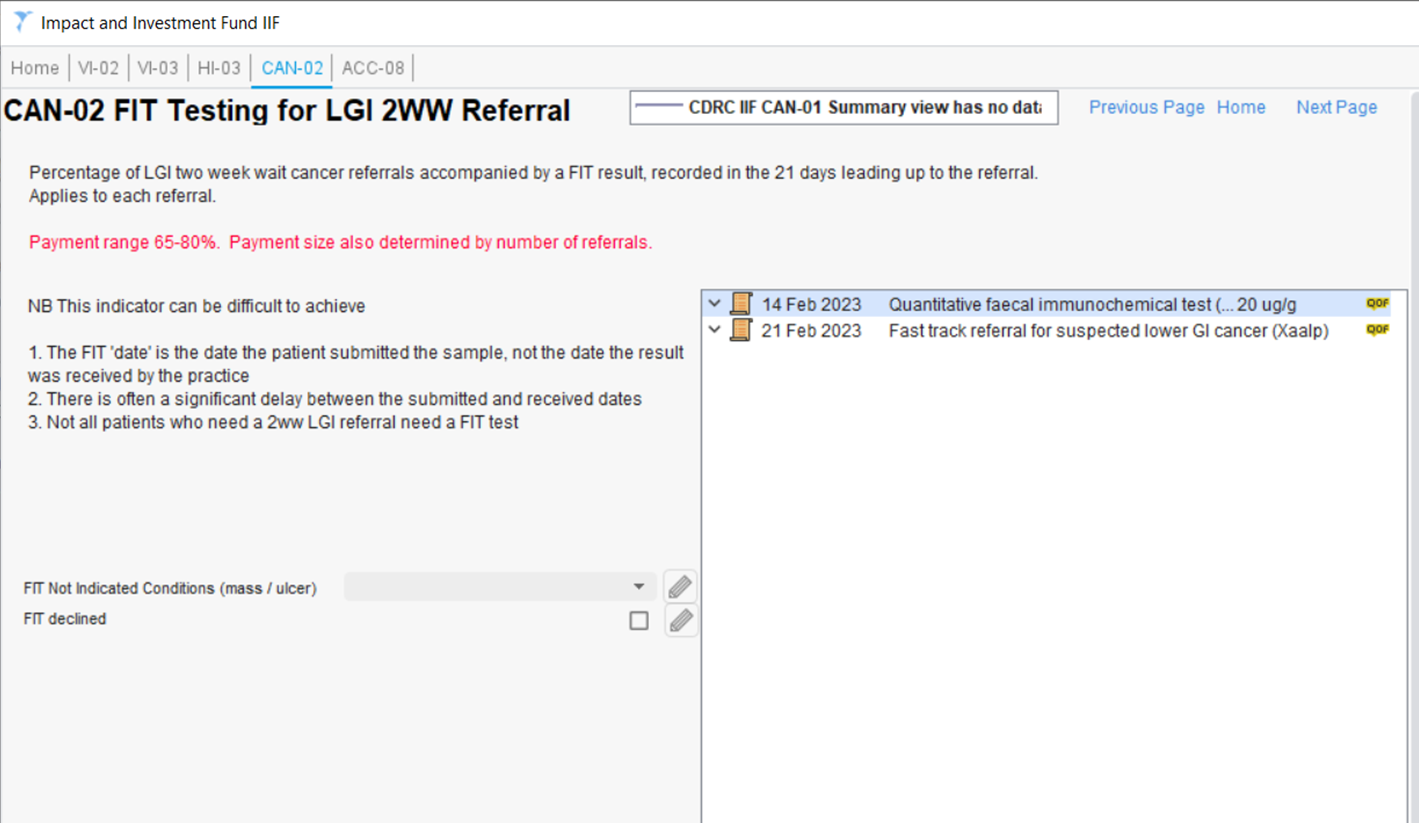
Percentage of lower gastrointestinal two week wait (fast track) cancer referrals accompanied by a faecal immunochemical test (FIT) result, with the result recorded in the 21 days leading up to the referral.
Payment Range: 65-80%
Payment size also determined by number of referrals.
Searches for this indicator are found in the CDRC Contracting > PCN DES folder:

The relevant information is shown on the CAN-02 tab of the ‘Impact and Investment Fund IIF’ template: