Accessing CDRC resources on SystmOne
To access the below resources you will need to be a member of the DCS group on SystmOne. To do this, please follow the instructions on the CDRC SystmOne Access webpage.
CDRC SystmOne resources to support the care of patients with Learning Disabilities
Learning Disability Reports
CDRC’s Case Finding reports can be useful to help validate your Learning Disability (LD) register.
These reports are located in the folder CDRC Quality > Learning Disability

| Report Name | Returns |
| ? LD 1.1 Case Finding – Newly included on QoF Code Lists after 2020 # | Patients that were added to the register in 2020 when the code list was updated |
| ? LD 1.2 Case Finding – Removed from QoF Code Lists after 2020 # | Patients that were removed from the register in 2020 when the code list was updated |
| ? LD 1.3 Case Finding – Code that might indicate LD # | Patients with a code that might suggest LD who are not on the LD register |
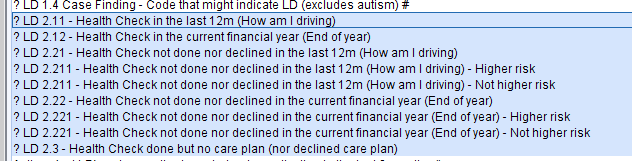
| ? LD 1.4 Case Finding – Code that might indicate LD (excludes autism) # | As for 1.3 but not including autism |
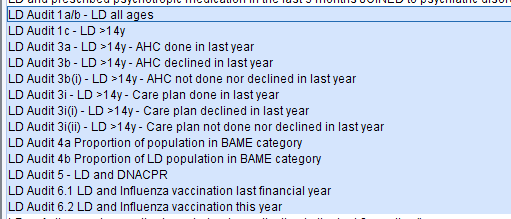
CDRC’s Health Check reports will identify patients who have had/ not had their annual review health check.
The reports to identify patients who have yet to have a check or opt out are subdivided into reports of those likely to be at ‘higher risk’. The criteria for higher risk are:
- Not had a health check for 2 years
- BMI <19 or >40
- More than one non-LD long term condition
- On antidepressants, antipsychotics, anxiolytics, gabapentinoids, hypnotics, lithium, opioids
- On medication where appropriate monitoring is significantly overdue
- Has a LTC with features of concern
- Has a PEG or history of aspiration pneumonia
Learning Disability Template
How to Access
With the Patient record retrieved, in the lower left hand corner there is a search bar, type in ‘Learning Disabilities CDRC’ and select the following template:

Alternatively, press F12 and type in ‘Learning Disabilities CDRC’ in the search bar, this will return the aforementioned template.
Learning Disability Template
The Learning Disability template is split into two main parts:
- A section where current information about the patient can be viewed and updated – below
- A section to facilitate a structured annual review in line with the LD Annual Review as set out in the DES national specification
The LD health check has been completely updated to integrate with other DCS care planning modules such as dementia, palliative care, avoiding unplanned admission etc.
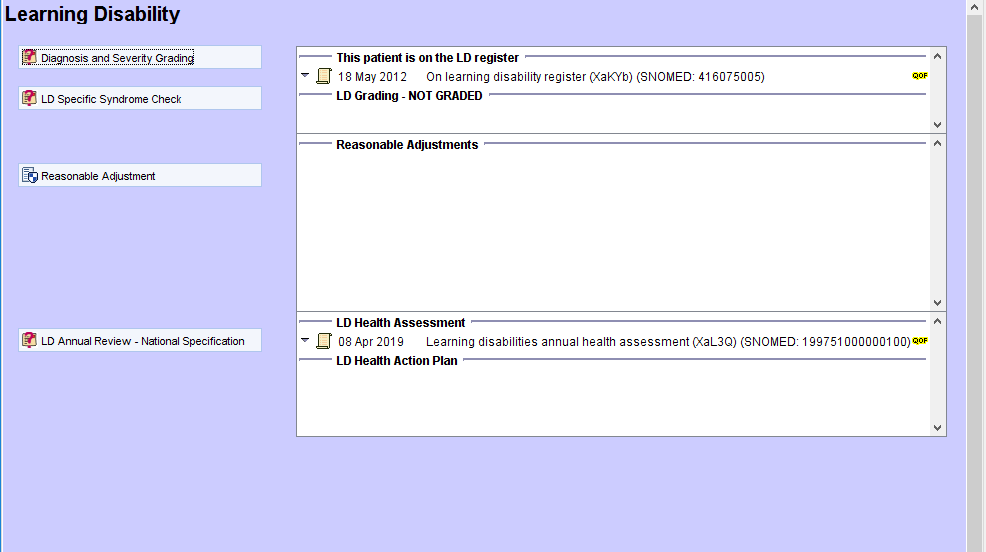
The Learning Disability Home Page provides a quick overview of the patient’s LD diagnosis codes, the date of the last LD review and action plan. There is a button to start the annual LD review. A link has been left to the old review template for those practices who wish to stick to that.
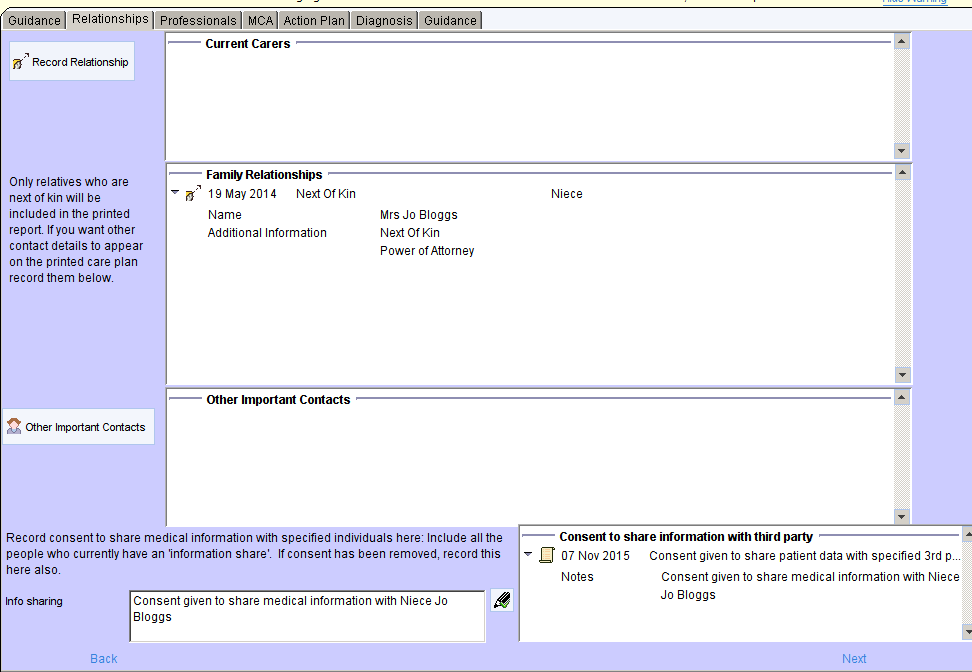
The Relationships Page is the same as all other care planning templates, providing details of relatives and carers and their details.
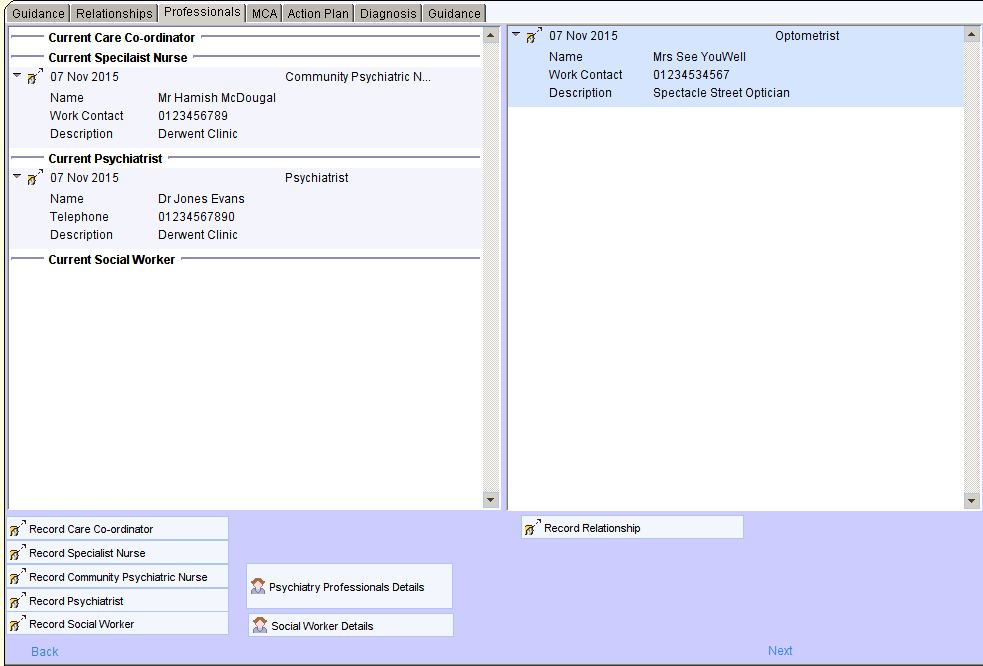
The Professionals Page is customised to provide greater prominence to relevant professionals such as psychiatrists, CPNs, social workers and care coordinators.
The Psychiatry Professionals and Social Worker Details buttons open screens that display more detailed information about these professionals, including previous relationships.
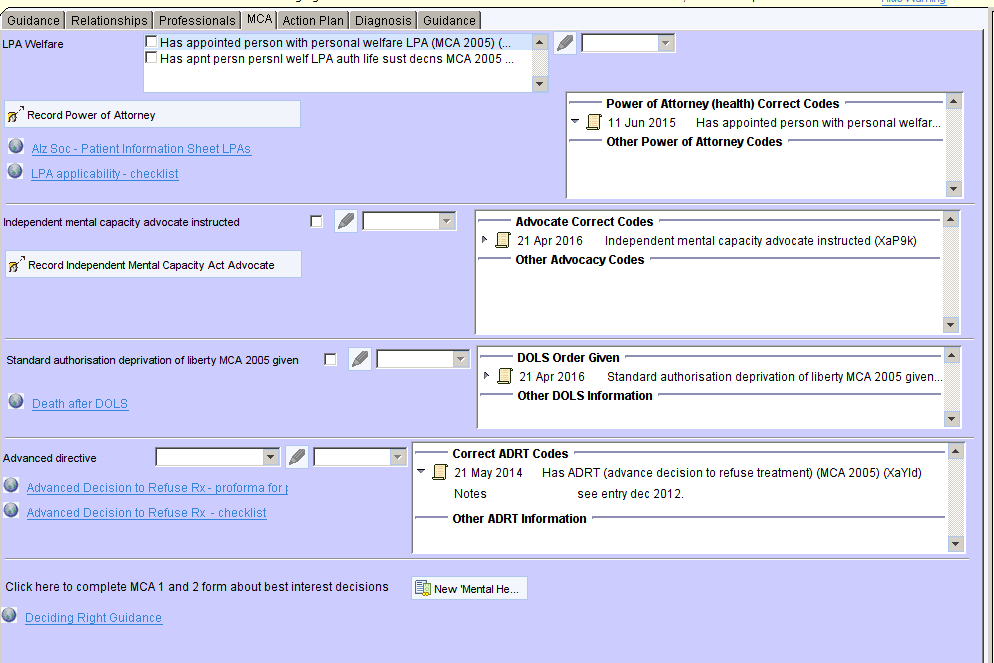
The MCA Page is identical to other care planning templates allowing users to view and amend information about power of attorney, IMCAs, advanced directives etc.
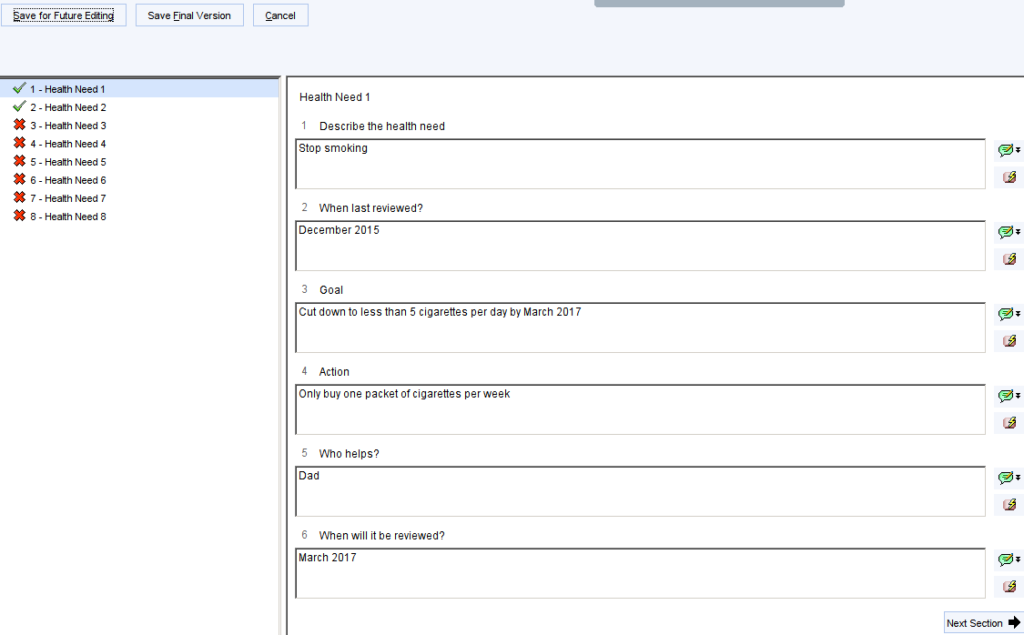
The Action Plan Page provides the ability to view and amend the current action plan and to record any other important information.
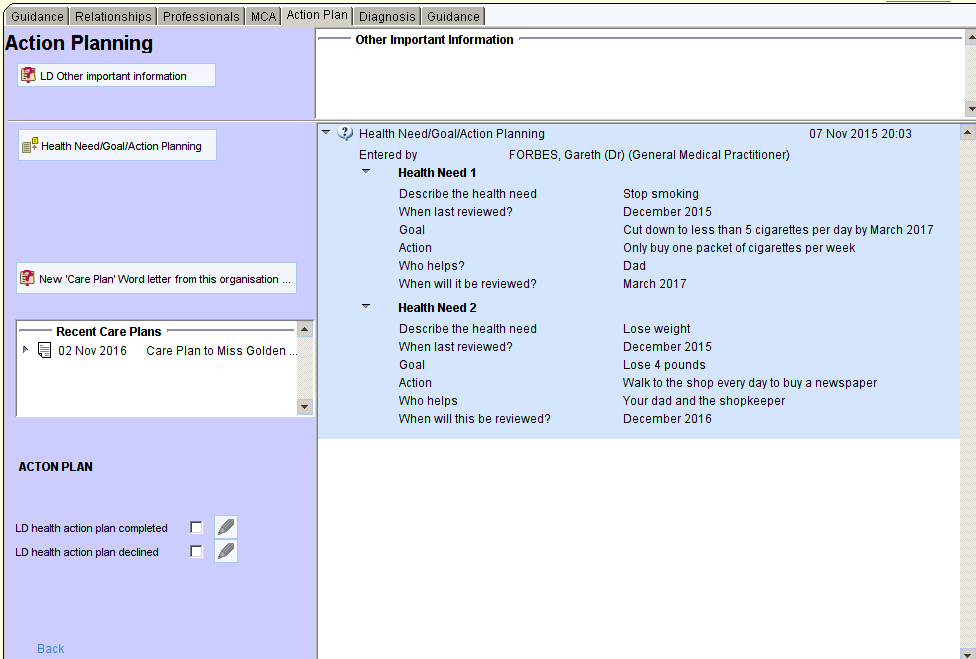
If the panels on the right are blank, click on the relevant button on the left to start a new action plan or ‘other important information’
If the panels already contain information that you wish to amend or update, right click anywhere in that panel, choose Copy Questionnaire, then choose Copy Comments.
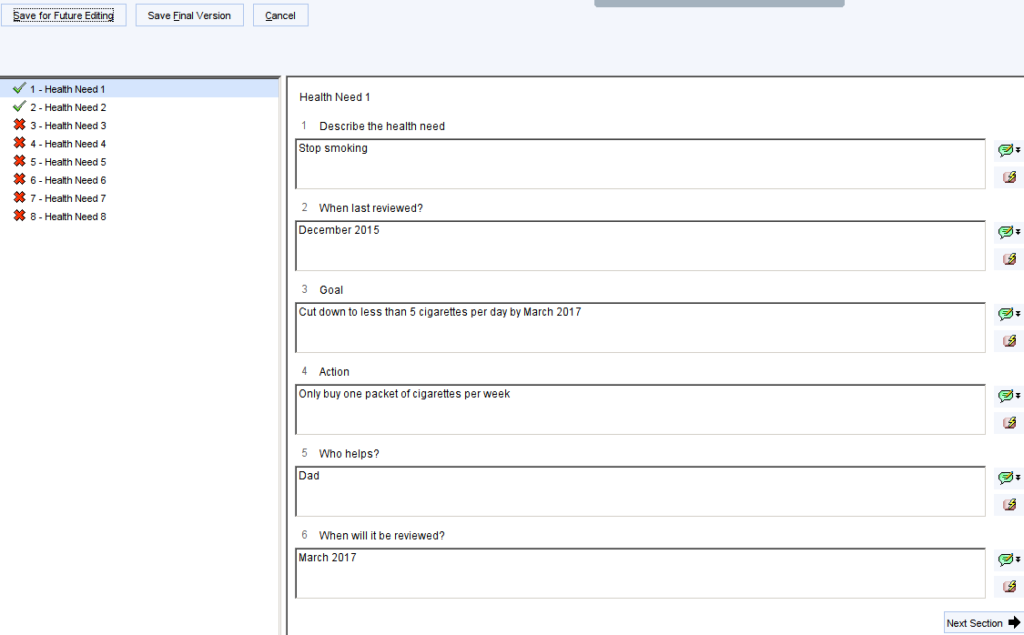
Complete the questionnaire then click Save Final Version when completed. You can record up to 8 different health needs.
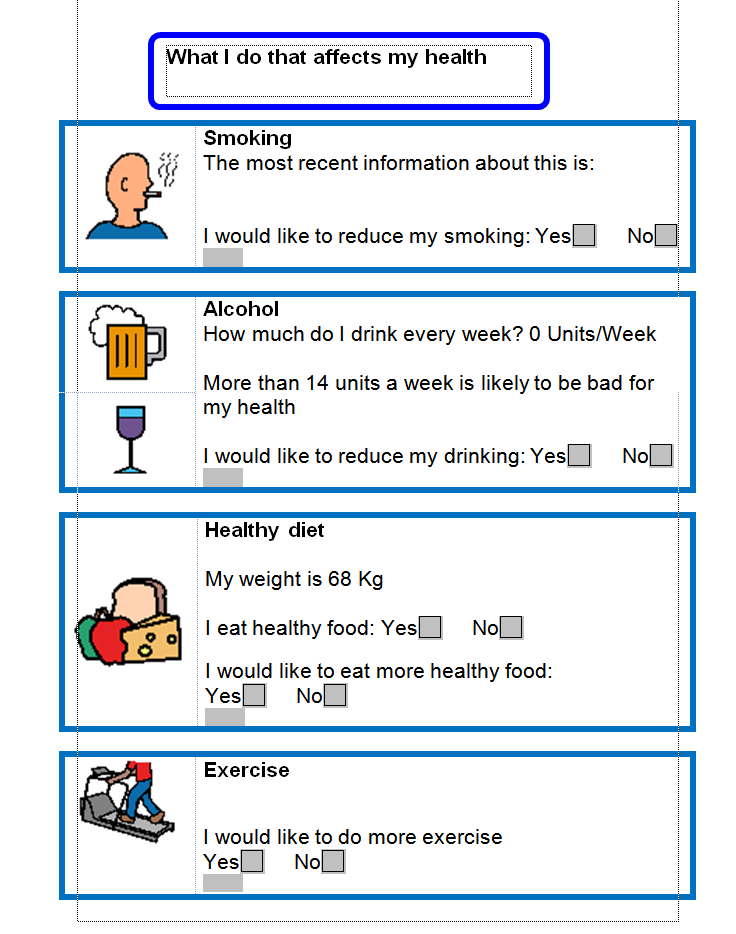
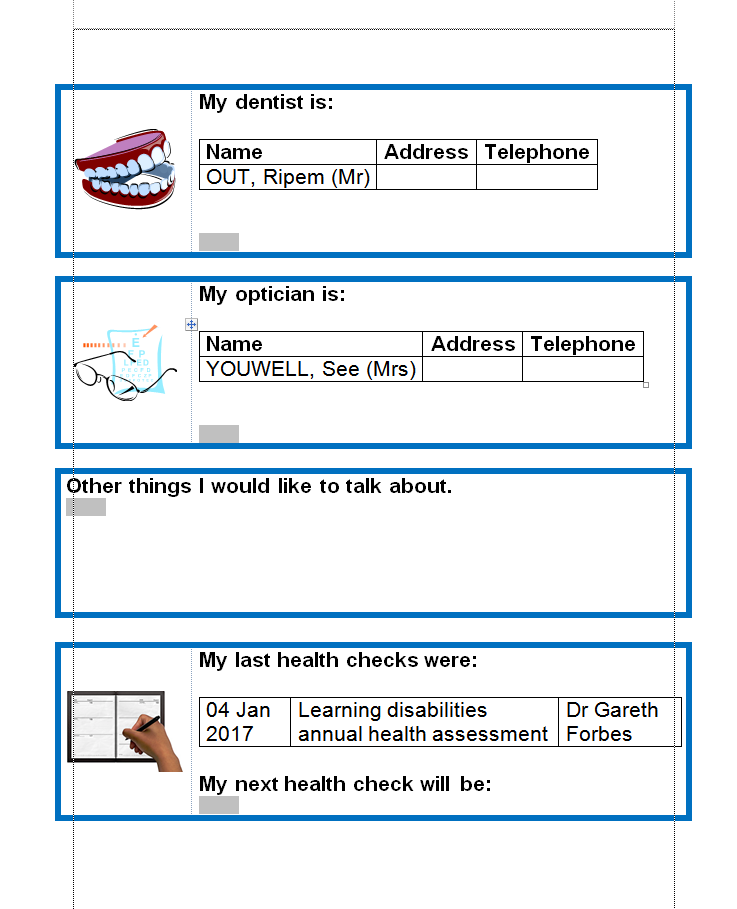
To create a paper document to give or email to the patient, click
Then choose Write Now. A prepopulated Action Plan will be created. An example action plan can be found here LD Action Plan
Previous Action Plans can be viewed from the Communications and Letters Node or by right clicking on the Recent Care Plans panel and choosing View Content.
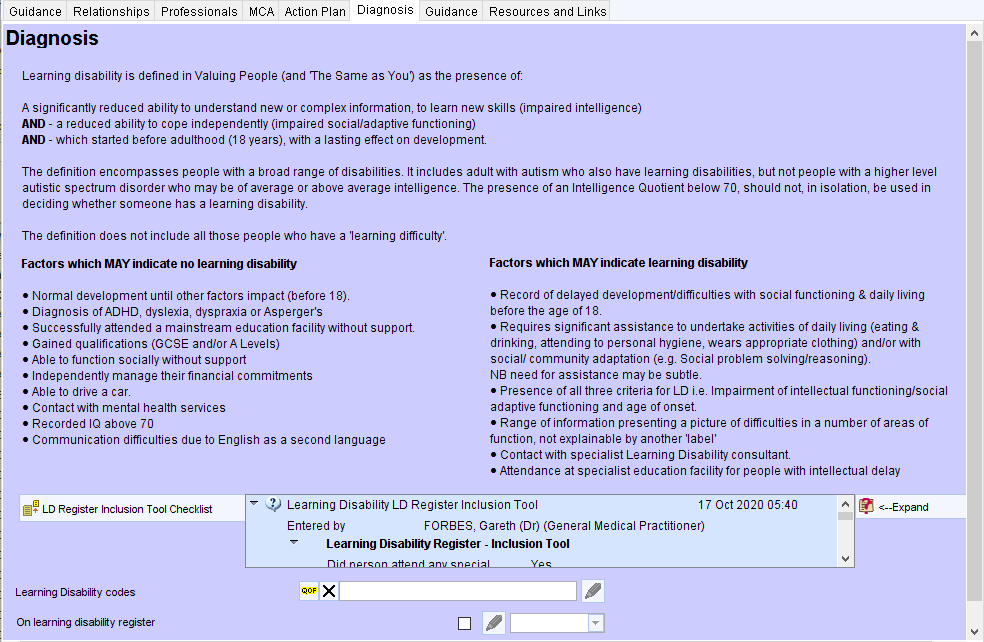
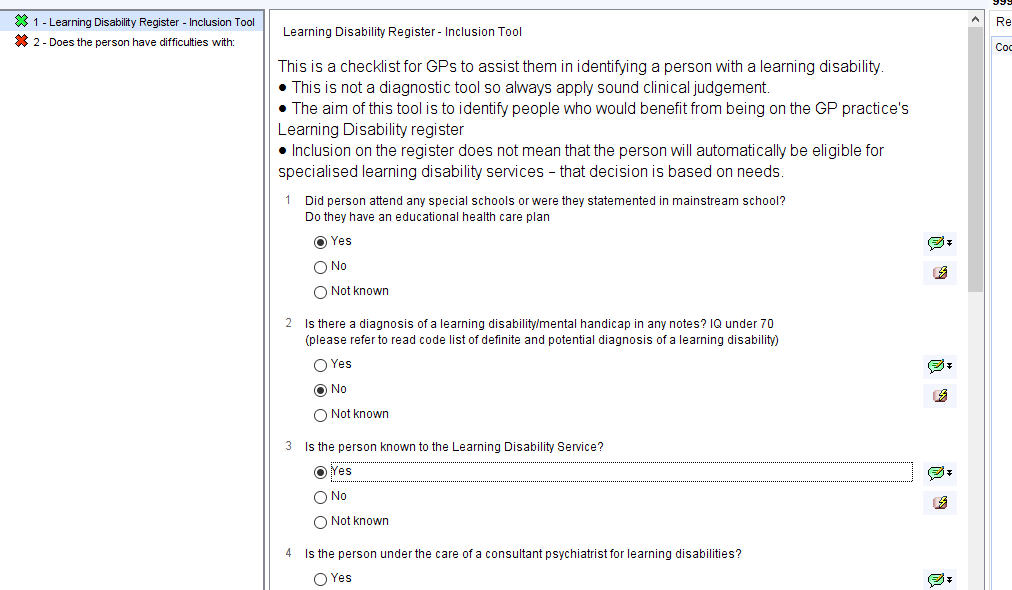
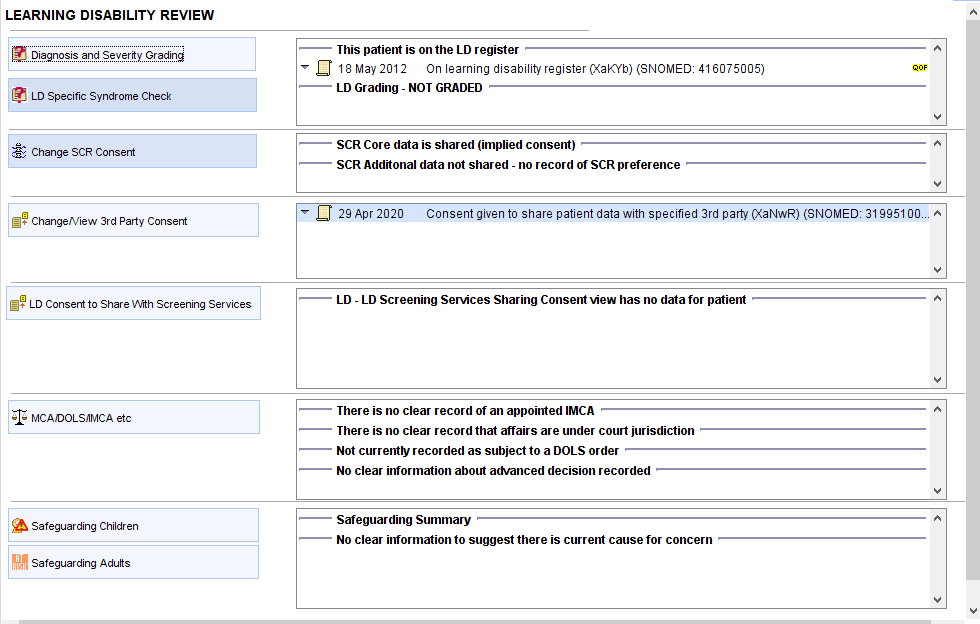
The Diagnosis Page shows the definition of learning disability. There is a LD Register inclusion checklist with a panel to show the last time this was completed. The <–Expand button can be used to show the full details of the most recently completed checklist.
Learning Disability Annual Review Template
How to Access
With the Patient record retrieved, in the lower left hand corner there is a search bar, type in ‘Learning Disability Annual Review CDRC’ and select the following template:

Alternatively, press F12 and type in ‘Learning Disability Annual Review CDRC’ in the search bar, this will return the aforementioned template.
Learning Disabilities Annual Review
The Learning Disability Annual Review part of the template facilitates a structured annual review.
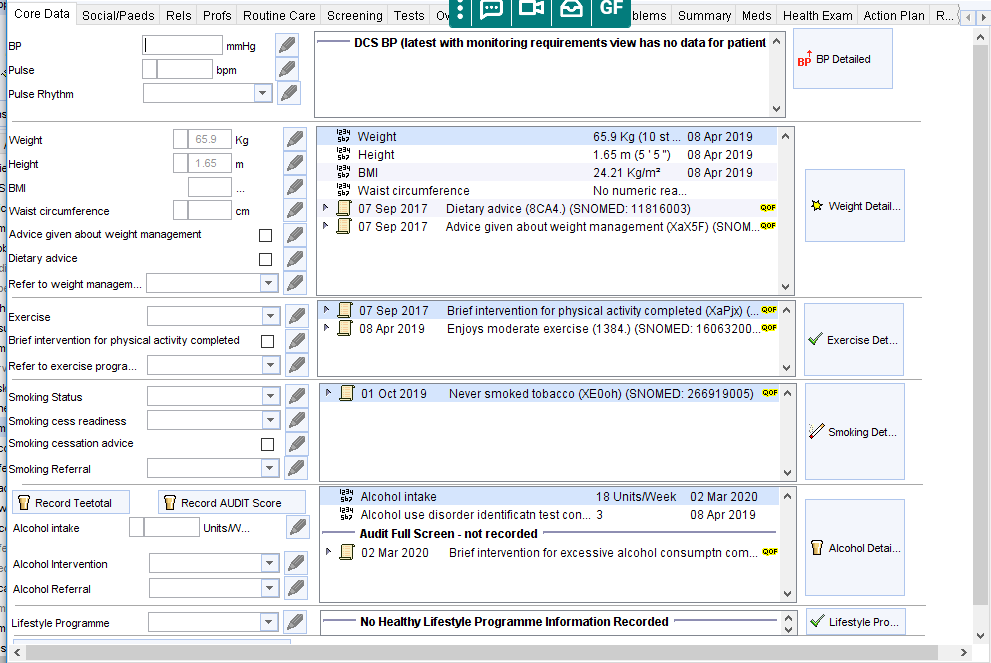
The Core Data Page allows recording of key measurements and lifestyle advice
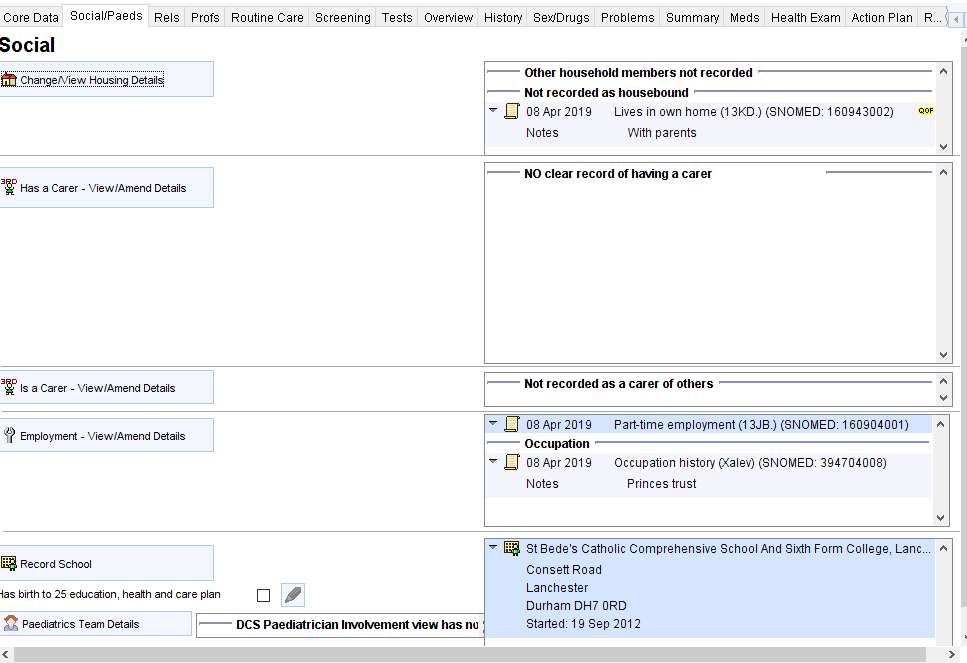
The Social/Paeds Page allows viewing, recording and editing of key social information such as accommodation, carers, employment and schooling.
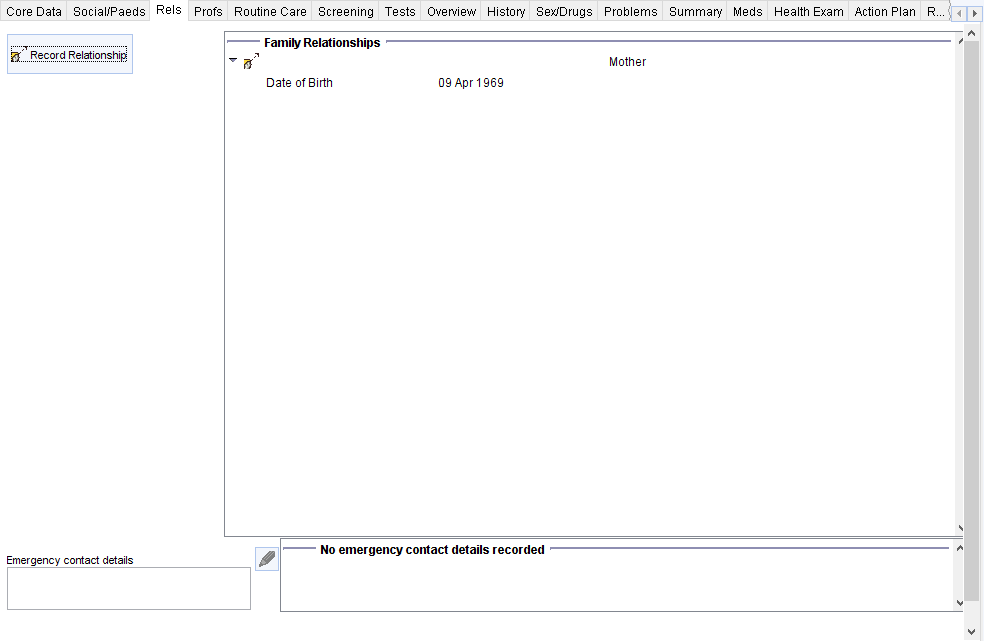
The Relationships Page allows recording of key family and friend relationships.
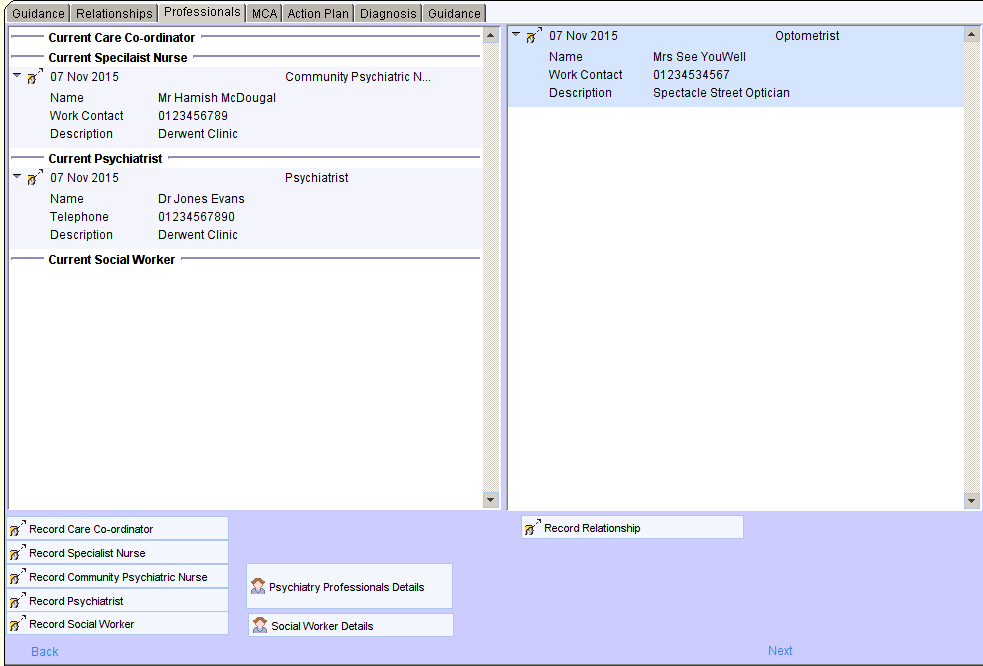
The Professionals Page is customised to provide greater prominence to relevant professionals such as psychiatrists, CPNs, social workers and care coordinators.
The Psychiatry Professionals and Social Worker Details buttons open screens that display more detailed information about these professionals, including previous relationships.
The Routine Care Page allows recording of information about dental and optometrist care, communication requirements, functional skills such as ADLs and recommended vaccinations.
The Screening Page shows relevant information for key screening programmes
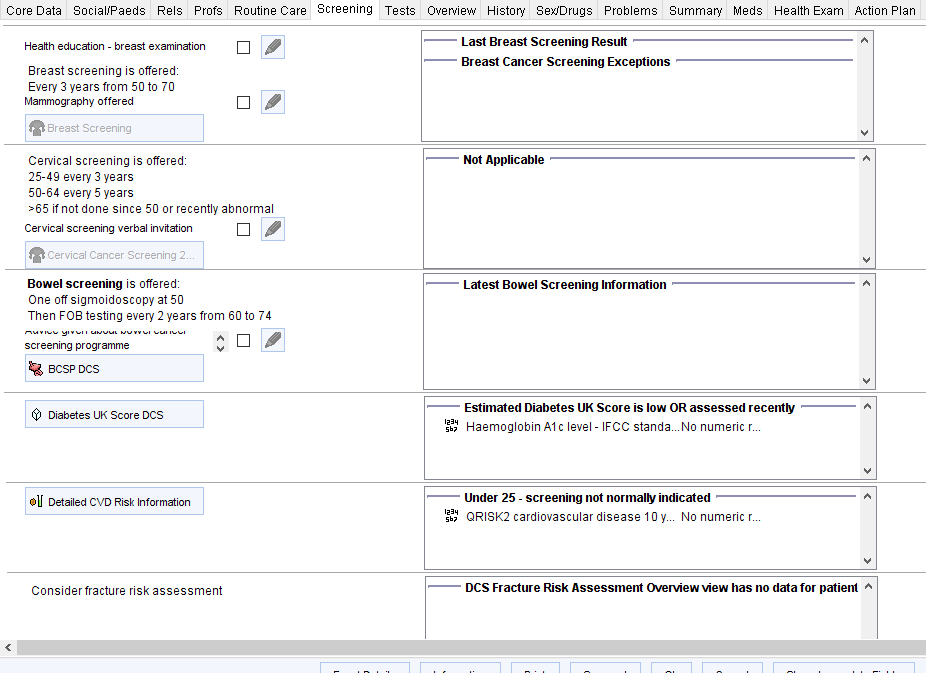
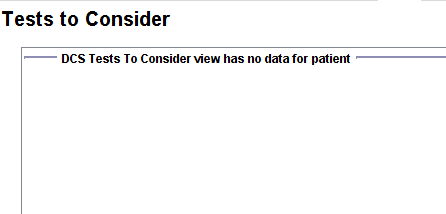
The Tests Page shows any tests that might be indicated based on current medication, long term conditions, recent results and screening recommendations.
The information in the sections above could largely be obtained by administration staff and/or health care assistants. Subsequent information is likely to need more experienced clinical input.
The Overview Page displays some key information
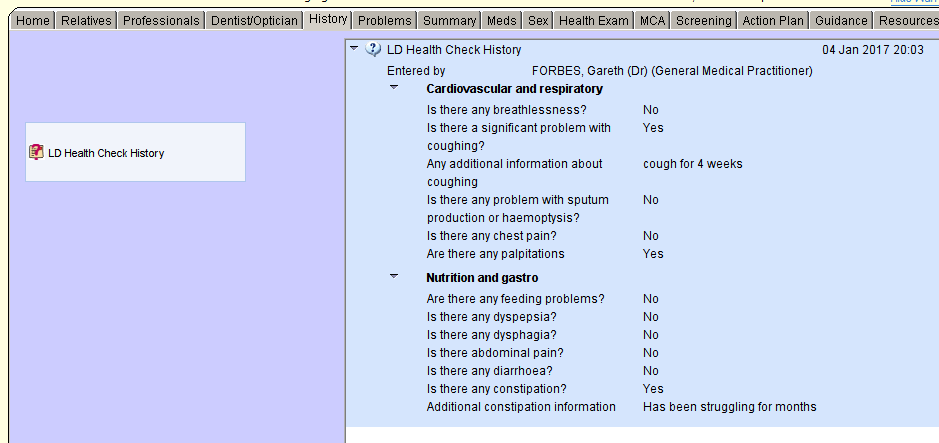
The History Page prompts the user to record a structured history using a questionnaire that expands to request more details automatically, if any issues are raised. Click Save Final Version once completed.
The most recent results of this history are displayed on the right hand panel.
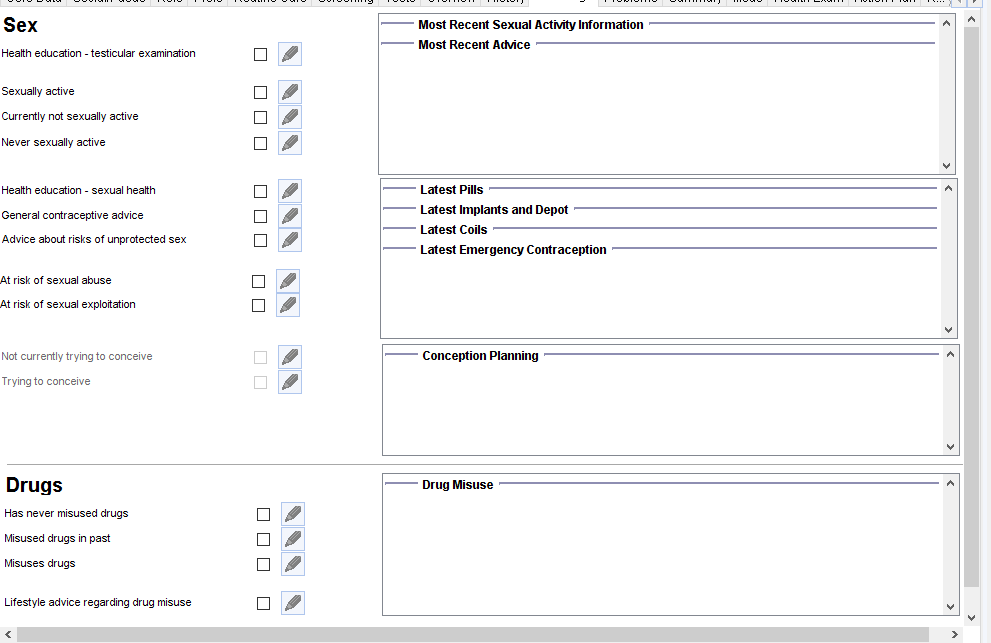
The Sex/Drugs Page allows recording of relevant information
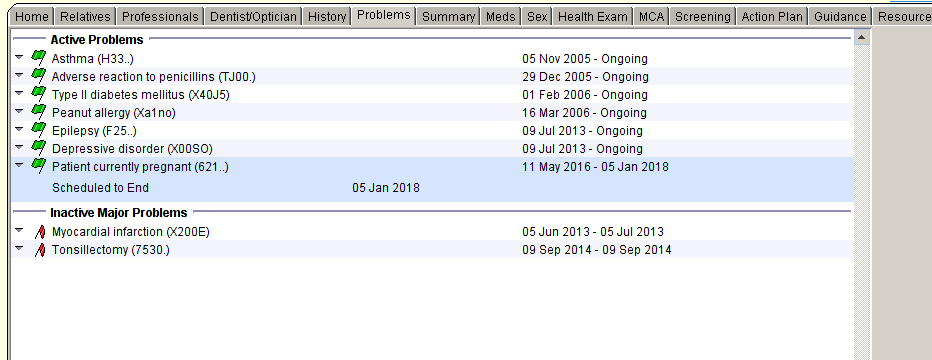
The Problem or Summary Pages (depending on practice preference) display the most recent problem lists which can be amended or updated by right clicking on the various entries.
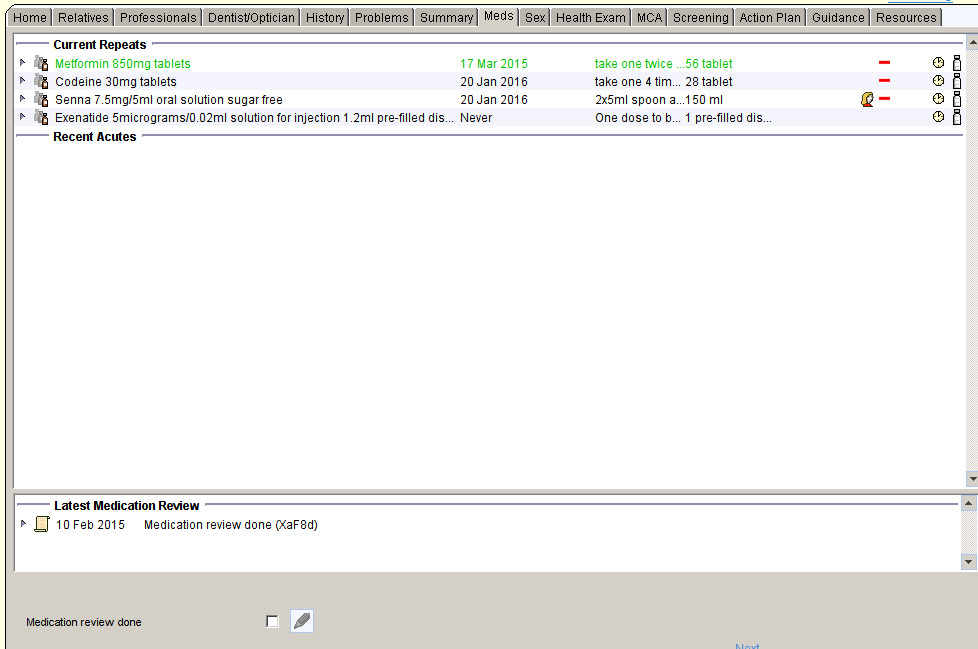
The Meds Page shows current medication
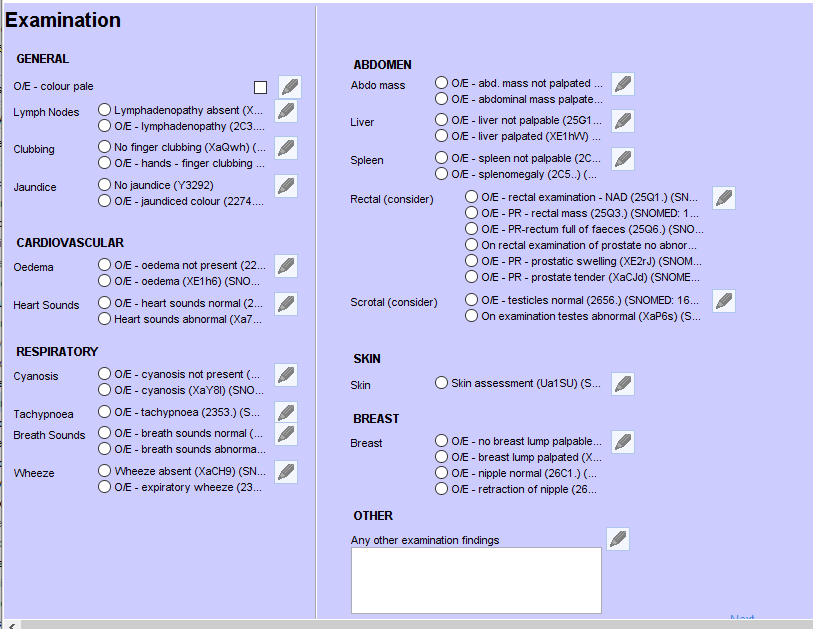
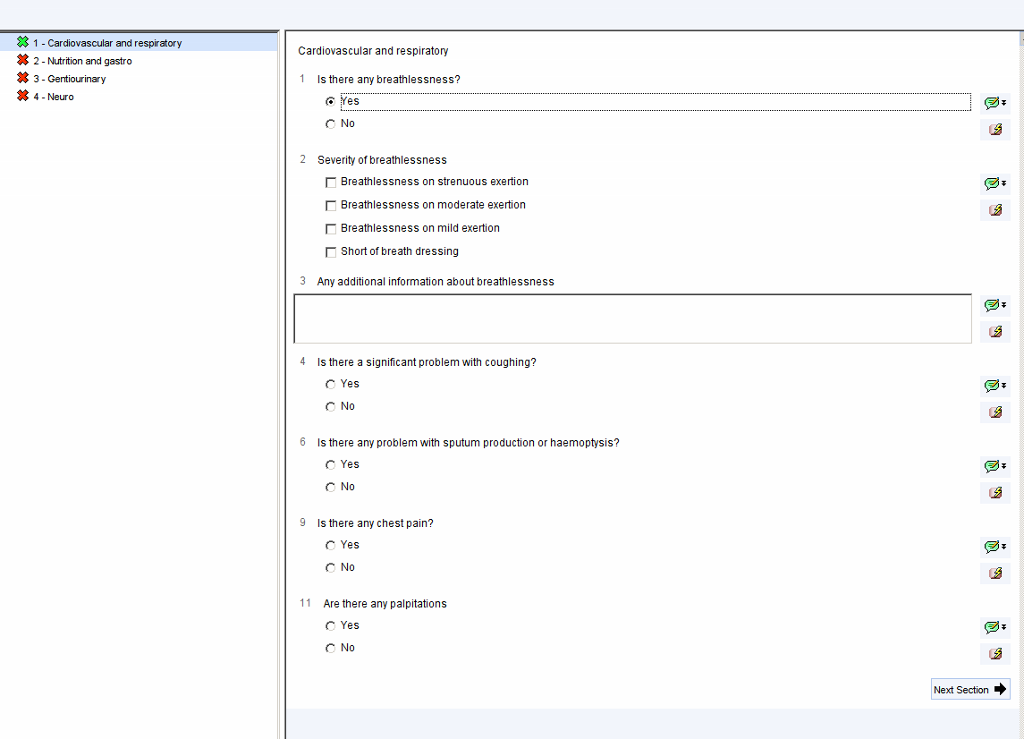
The Health Exam Page facilitates a structured examination based on the Cardiff model.
The Action Plan Page provides the ability to view and amend the current action plan and to record any other important information.
If the panels on the right are blank, click on the relevant button on the left to start a new action plan or ‘other important information’
If the panels already contain information that you wish to amend or update, right click anywhere in that panel, choose Copy Questionnaire, then choose Copy Comments.
Complete the questionnaire then click Save Final Version when completed. You can record up to 8 different health needs.
To create a paper document to give or email to the patient, click
Then choose Write Now. A prepopulated Action Plan will be created. An example action plan can be found here LD Action Plan
Previous Action Plans can be viewed from the Communications and Letters Node or by right clicking on the Recent Care Plans panel and choosing View Content.
Additional Resources
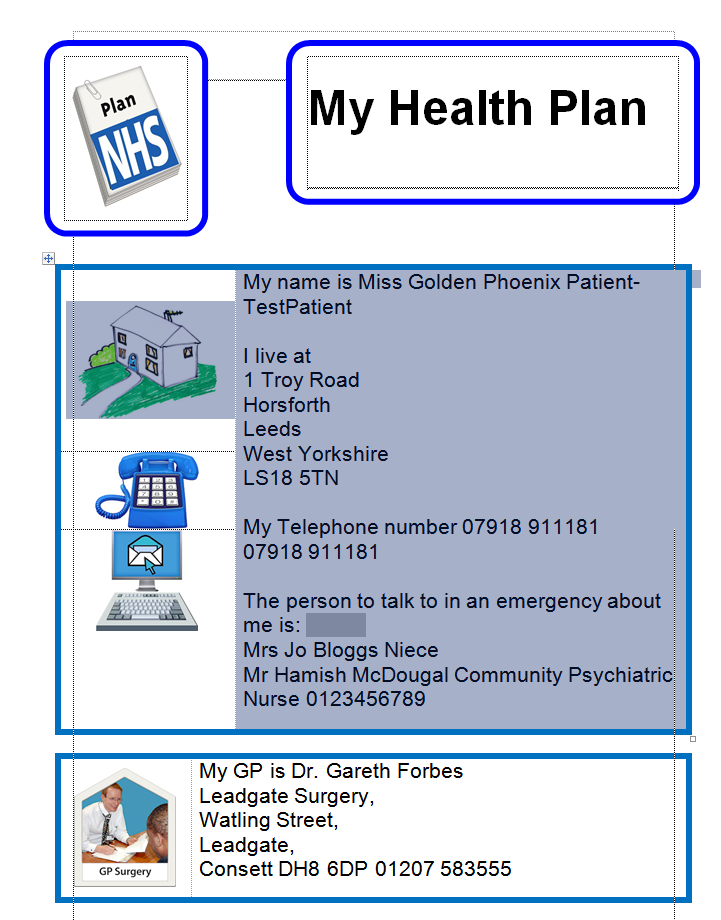
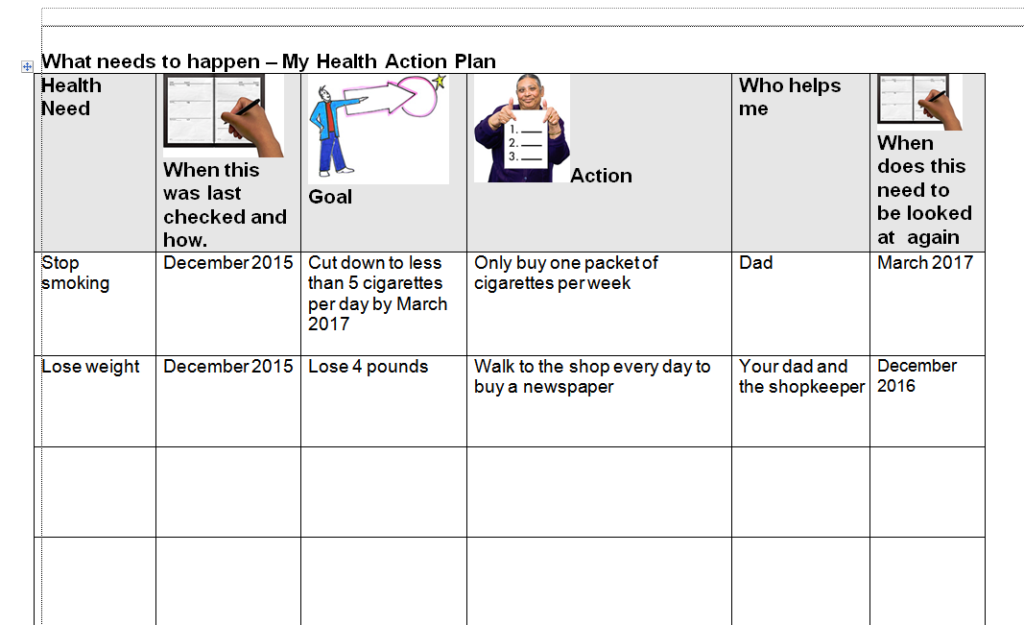
Learning Disability Action Plan
The LD Action Plan, prepopulates information from the LD template. The plan can then be further customised in the grey boxes (or anywhere else)
Quality Improvement
The following resources will help with quality improvement related to care of patients with a learning disability
RCGP Toolkit – https://www.rcgp.org.uk/clinical-and-research/resources/toolkits/health-check-toolkit.aspx
NHS Tool for quality checking LD Health Checks:
The following searches can be used to complete the information needed in the documents above