A suite of Population Reporting searches for EMIS, created by the CDRC can be used identify patients in your practice who might benefit from lipid lowering or optimisation of treatment.
To enable actioning of these Population Reporting searches with guided instruction for patient care, please use the CDRC Lipid Management Template which can be accessed using the CDRC Precision Launcher. This holistic tool allows for accurate assessment, coding and management of patients to help meet best practice, QoF and PCN DES IIF indicators.
Accessing the Population Reporting Searches
To access the CDRC Lipids Population Reporting Searches on EMIS, you will need to download and import the following .zip file:
If you have not performed this process before, please refer to the Download/ Import guide below, which provides you with step-by-step instructions on how to Download and Import .zip files into EMIS:
You can check whether you have the most up-to-date version by reviewing the date on the .zip file. Any updates to the Population Reporting searches will be communicated to CDRC Precision users via the mailing list for the CDRC. To ensure you stay up to date with the latest information, please sign up to the mailing list at http://eepurl.com/9131L
Guidance on the Population Reporting Searches
To view CDRC’s focused Population Reporting Lipid searches navigate to the CDRC Quality Lipids (23rd October 2023) folder and open the CDRC Quality Lipids Focused Reports folder.

The Focused Population Reporting Lipids searches in this folder are highlighted below along with information that explains the patients that these searches return and possible actions to take.
Lipid Screening – Screening for people at risk of CVD
| Report Name | Report Returns |
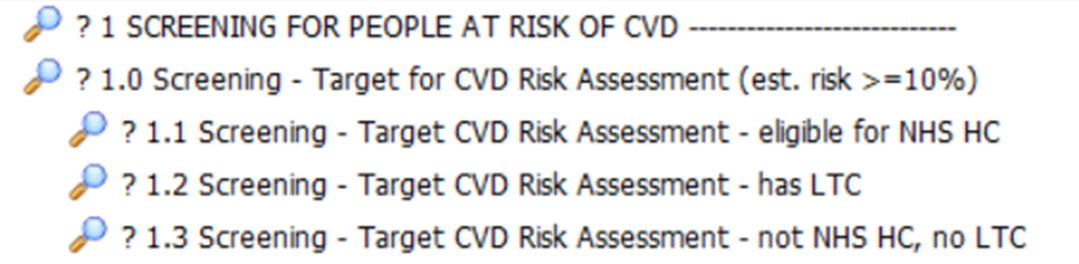
| ? 1.0 Screening – Target CVD Risk Assessment (estimated risk is >10%) | Patients who have an estimated QRisk2 calculated (un-coded) who may be eligible for a targeted CVD Risk assessment. |
| ? 1.1 Screening – Target CVD Risk Assessment – eligible for NHS Health check | Patient’s included in report 1.0 that you could recall for an NHS Health Check. |
| ? 1.2 Screening – Target CVD Risk Assessment – has LTC | Patient’s included in report 1.0 that you could recall for an LTC review (excluding respiratory reviews). |
| ? 1.3 Screening – Target CVD Risk Assessment – not NHS Health check or LTC | Patient’s included in report 1.0 excluding those that could be invited for an NHS Health Check or an LTC review. These patients could potentially be missed from any routine recall but existing coding in their record suggests they have a QRisk2 >10%. |
Lipid Screening – Screening for Familial Hypercholesterolaemia
| Report Name | Report Returns |
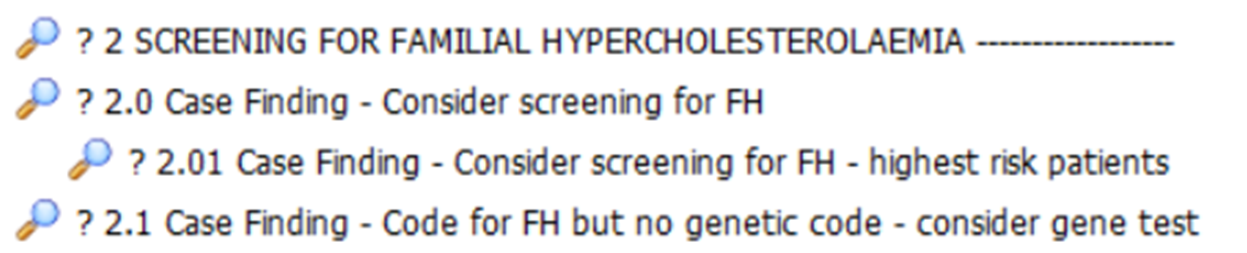
| ? 2.0 Case Finding – Consider screening for familial hypercholesterolaemia | Patients who may have familial hypercholesterolaemia based on the DLCN criteria, Simon Broome and NICE Plus criteria. |
| ? 2.01 Case Finding – Consider screening for FH – highest risk patients | Patients included in the report 2.0 with the highest risk scores that are most likely to have FH. |
| ? 2.1 Case Finding – Code for FH but no genetic code – consider gene test | Patients that have a possible/probable/FH code who do not have a genetic FH code diagnosis. These patients should be reviewed and genetic code added, or referral made, or removal of FH code if incorrect (e.g. Patient has secondary hyperlipidaemia). |
Lipid Management – Consider Starting / Restarting Lipid Lowering
| Report Name | Report Returns |
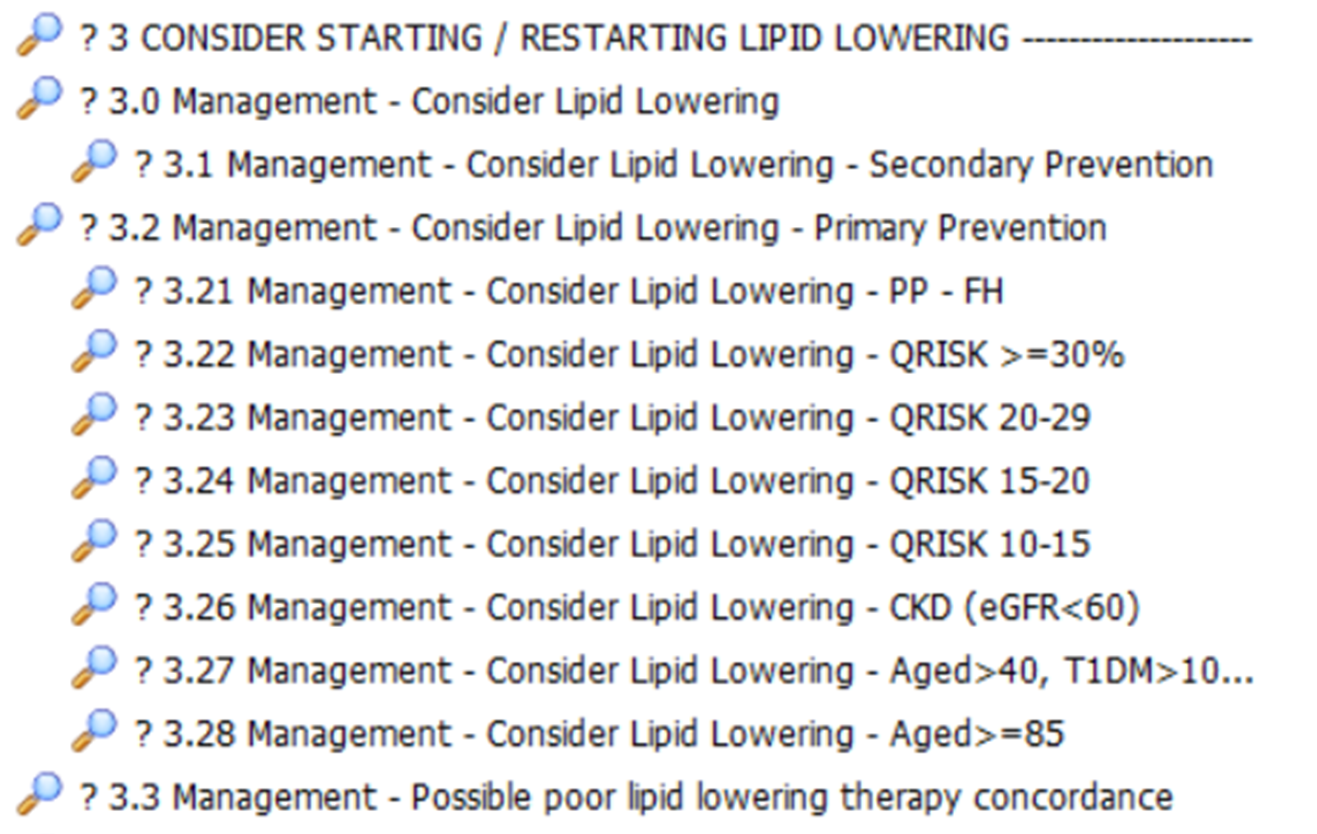
| ? 3.0 Management – Consider Lipid Lowering | Patients who appear eligible for lipid lowering for primary or secondary prevention who don’t have a recorded reason why not |
| ? 3.1 Management – Consider Lipid Lowering – Secondary Prevention | Patients with manifest atherosclerosis who are not taking lipid lowering medication with no clear indication why. |
| ? 3.2 Management – Consider Lipid Lowering – Primary Prevention | Patients with coded reasons to be on lipid lowering medication who are not. There are further subdivisions of this report, as shown in the screenshot above, that identify specific patient cohorts.. |
| ? 3.3 Management – Possible poor lipid lowering therapy concordance | Patient’s who are prescribed lipid lowering medication, but they have not had an issue in the last 3 months. |
Lipid Management – Lipid Lowering Optimisation
| Report Name | Report Returns |
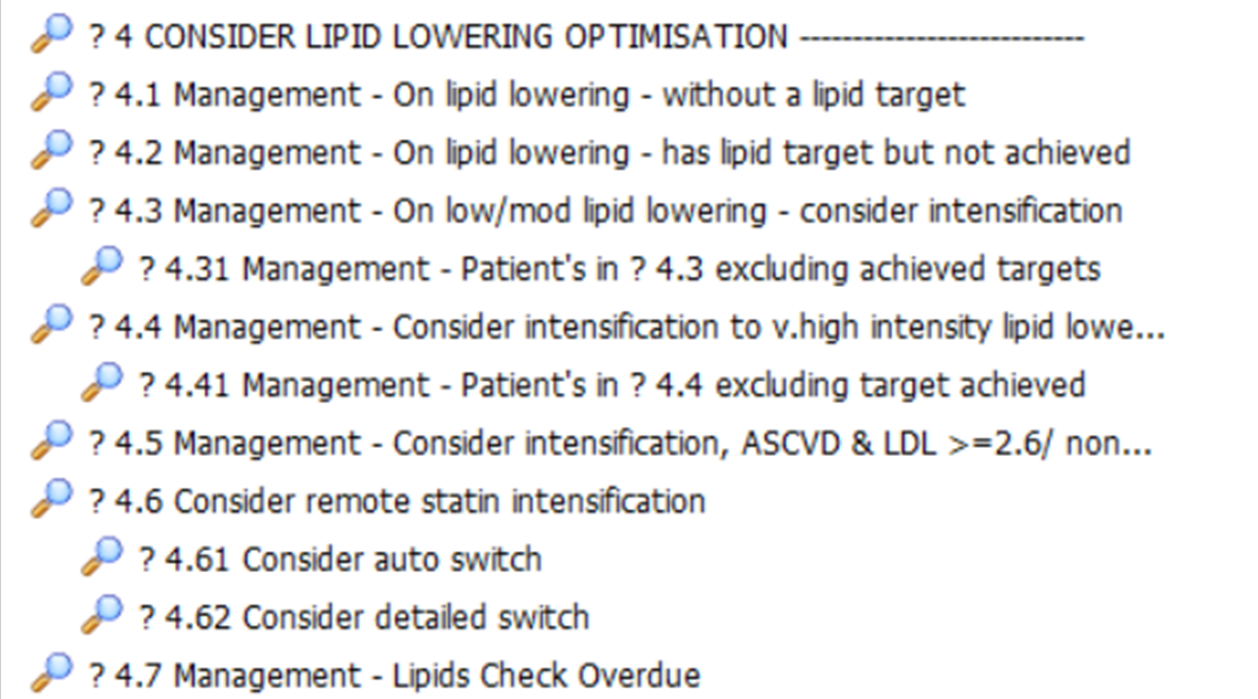
| ? 4.1 Management – On lipid lowering – without a target | Patients with repeat lipid lowering therapy who do not have a lipid target. |
| ? 4.2 Management – On lipid lowering – has lipid target but not achieved | Patients with a lipid target which has not been achieved. |
| ? 4.3 Management – On low/mod lipid lowering – consider intensification | Patients on moderate or low potency lipid lowering without a documented reason. |
| ? 4.31 Management – Patient’s in ? 4.3 excluding achieved targets | As for 4.3 but excludes patients who have reached their target cholesterol. |
| ? 4.4 Management – Consider intensification to v.high intensity lipid lowering | Patients eligible for secondary prevention who are not on very high intensity lipid lowering. |
| ? 4.41 Management – Patient’s in ? 4.3 excluding achieved targets | As for 4.4 but excluding patients who have reached their target cholesterol. |
| ? 4.5 Management – Consider intensification, ASCVD & LDL >=2.6/ nonHDL >=2.5 | Patients with ASCVD with LDL >=2.6 or Non HDL >=2.5 |
| ? 4.6 Consider remote statin intensification | |
| ? 4.61 Consider auto switch | |
| ? 4.62 Consider detailed switch | |
| ? 4.7 Management – Lipids Check Overdue | Patients who have not had a lipid check in the last 15 months. |
Lipid Management – May Need Specialist Lipid Management
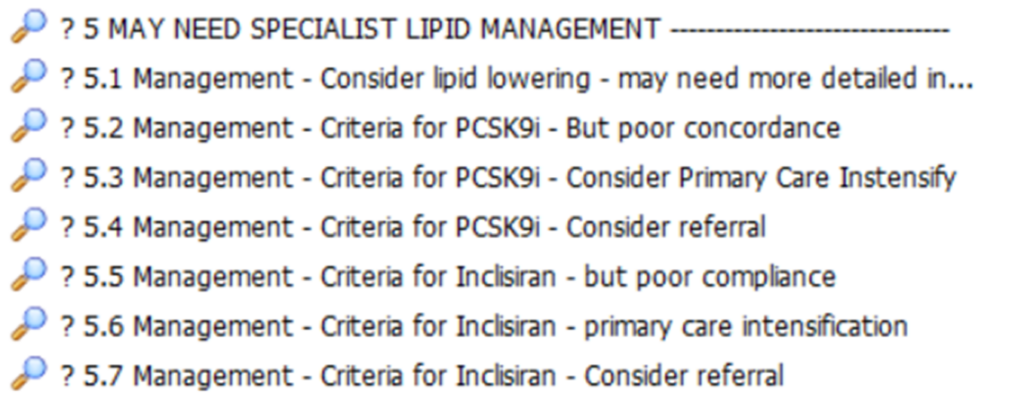
| Report Name | Report Description |
| ? 5.1 Management – Consider lipid lowering – may more detailed input | Patients who appear to need lipid lowering but have had ADR to at least one statin AND ezetimibe – may need specialist input |
| ? 5.2 Management – Referral criteria for PCSK9i but poor concordance with current treatment | Fulfil referral criteria for PCSK9i therapy but may not be taking current lipid lowering therapy |
| ? 5.3 Management – Referral Criteria for PCSK9i – Consider primary care intensification | Fulfil referral criteria for PCSK9i therapy but there may be scope for intensification of lipid lowering therapy in primary care |
| ? 5.4 Management – Referral Criteria for PCSK9i – Consider referral | Likely to be eligible for PCSK9i referral |
| ? 5.5 Management – Referral criteria for Inclisiran but poor concordance with current treatment | Fulfil referral criteria for Inclisiran therapy but may not be taking current lipid lowering therapy |
| ? 5.6 Management – Referral Criteria for Inclisiran – Consider primary care intensification | Fulfil referral criteria for Inclisiran therapy but there may be scope for intensification of lipid lowering therapy in primary care |
| ? 5.7 Management – Referral Criteria for Inclisiran – Consider referral | Likely to be eligible for Inclisiran referral |
Lipid Management – Primary Prevention
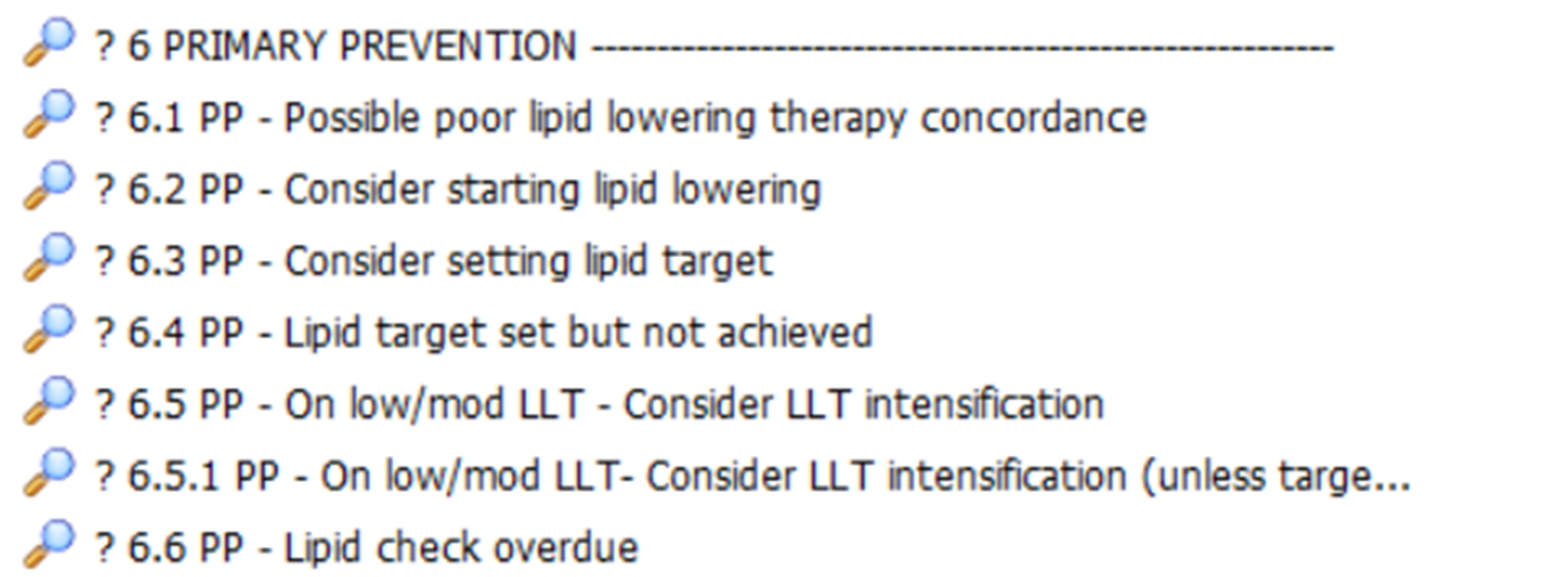
| Report Name | Report Returns |
| ? 6.1 PP – Possible poor lipid lowering therapy concordance | Patients with repeat lipid lowering who have not been issued a prescription in the last 3 months. |
| ? 6.2 PP – Consider starting lipid lowering | Patients who appear eligible for lipid lowering for primary and secondary prevention who don’t have recorded reason why not. |
| ? 6.3 PP – Consider setting lipid target | Patients with repeat lipid lowering therapy who do not have a lipid target. |
| ? 6.4 PP – Lipid target set but not achieved | Patients with a lipid target which has not been achieved. |
| ? 6.5 PP – On low/mod LLT – Consider LLT intensification | Patients on low or moderate potency lipid lowering without a documented reason. |
| ? 6.51 PP – On low/mod LLT – Consider LLT intensification (unless target already achieved) | As for 6.5 but excludes patients who have reached their target cholesterol. |
| ? 6.P pp – Lipid check overdue | Patients who have not had a lipid check in the last 15 months |
Lipid Management – Secondary Prevention
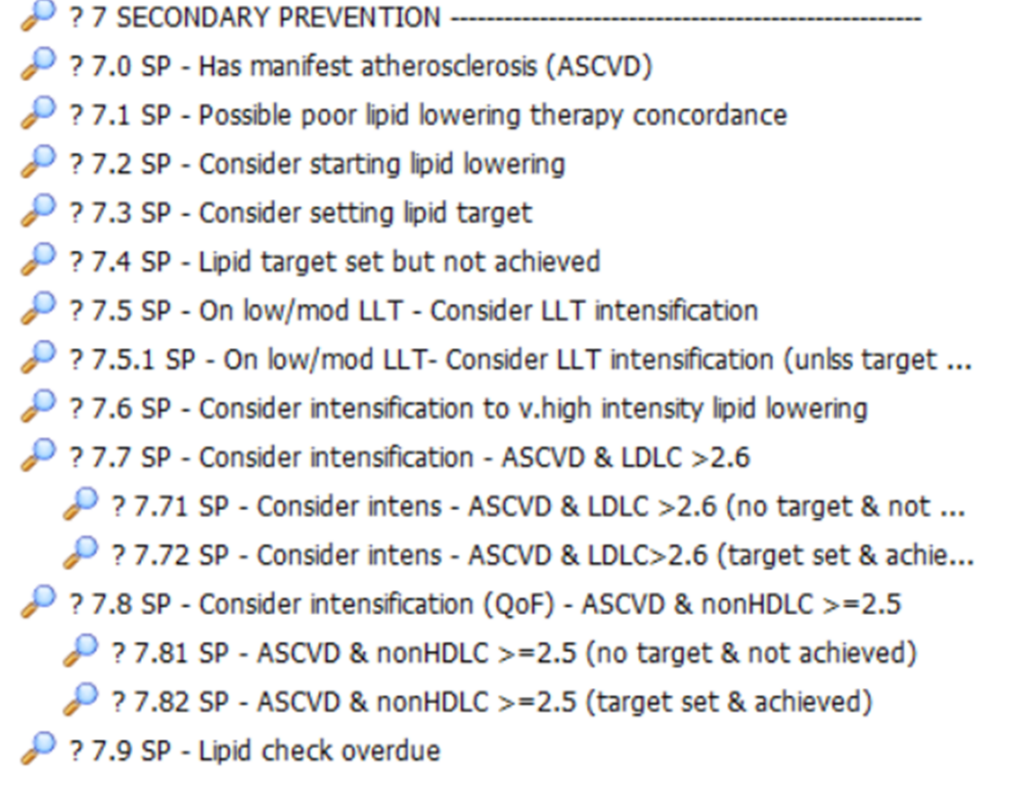
| Report Name | Report Returns |
| ? 7.0 SP – Has manifest atherosclerosis (ASCVD) | All ASCVD coded patients. |
| ? 7.1 SP – Possible poor lipid lowering therapy concordance | Patients with repeat lipid lowering who have not been issued a prescription in the last 3 months. |
| ? 7.2 SP – Consider starting lipid lowering | Patients who appear eligible for lipid lowering for primary and secondary prevention who don’t have recorded reason why not. |
| ? 7.3 SP – Consider setting lipid target | Patients with repeat lipid lowering therapy who do not have a lipid target. |
| ? 7.4 SP – Lipid target set but not achieved | Patients with a lipid target which has not been achieved |
| ? 7.5 SP – On low/mod LLT – Consider LLT intensification | Patients on low or moderate potency lipid lowering without a documented reason. |
| ? 7.5.1 SP – On low/mod LLT- Consider LLT intensification (unlss target achvd) | As for 7.5 but excludes patients who have reached their target cholesterol |
| ? 7.6 SP – Consider intensification to v.high intensity lipid lowering | Patients eligible for secondary prevention who are not on very high intensity lipid lowering. |
| ? 7.7 SP – Consider intensification – ASCVD & LDLC >2.6 | Patients with ASCVD with LDLC >=2.6 or Non HDLC >=2.5 |
| ? 7.71 SP – Consider intens – ASCVD & LDLC >2.6 (no target & not achieved) | As for 7.7 but excluding patients who have a lipid target and have achieved this target. |
| ? 7.72 SP – Consider intens – ASCVD & LDLC>2.6 (target set & achieved) | As for 7.7 but including patients who have a lipid target and have achieved this target. |
| ? 7.8 SP – Consider intensification (QoF) – ASCVD & nonHDLC >=2.5 | Patients with ASCVD & a Non HDLC >=2.5 |
| ? 7.81 SP – ASCVD & nonHDLC >=2.5 (no target & not achieved) | As for 7.8 but excluding patients who have a lipid target and have achieved this target. |
| ? 7.82 SP – ASCVD & nonHDLC >=2.5 (target set & achieved) | As for 7.8 but including patients who have a lipid target and have achieved this target. |
| ? 7.9 SP – Lipid check overdue | Patients who have not had a lipid check in the last 15 months |
CDRC Lipid Management Template
The Lipid Management Template is an intelligent template that helps guide clinicians through their patient’s lipid management, presenting relevant information depending on whether it is for primary prevention, secondary prevention and whether or not they are at target.
To access the CDRC Lipid Management Template, you will need to have the CDRC Precision Resource Launcher enabled at your practice. Information on how to do this can be found by clicking on the link below:
Once enabled, you will be able to follow these steps:
- With the identified patient’s record retrieved, press F12 and select CDRC Precision Resource Launcher which will open the following pop-up:
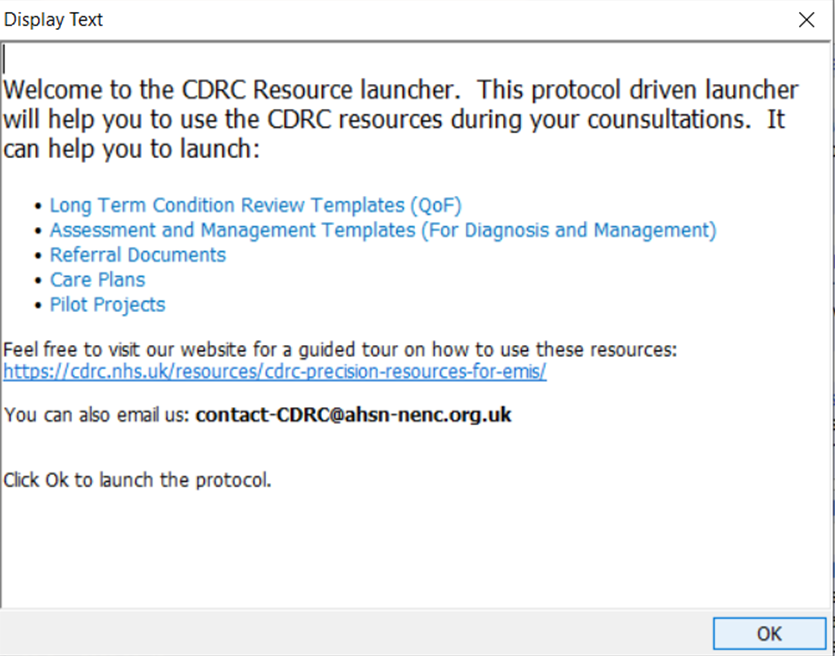
- Click ‘OK’
- Click on Assessment and Management Templates > Cardiovascular > Lipids Management, which will open the following template:
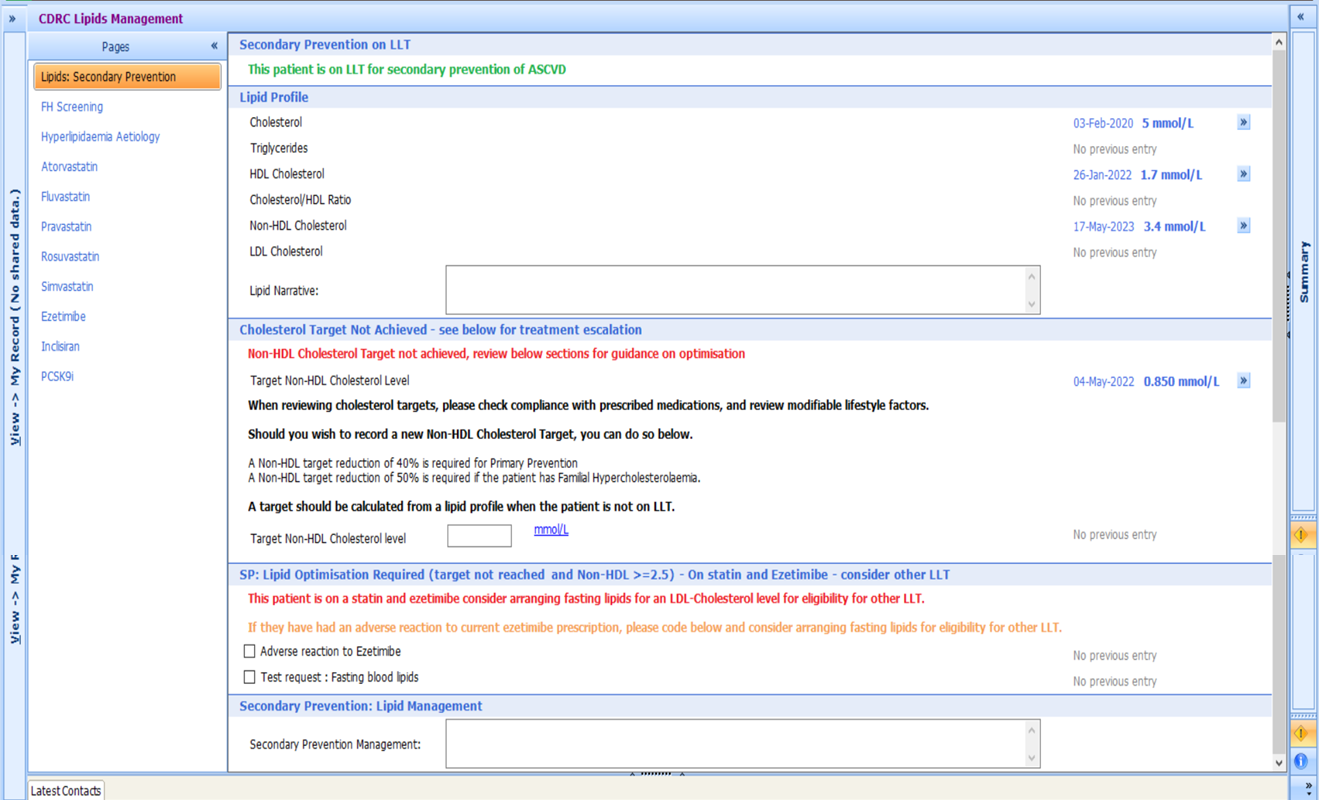
This screenshot is for a dummy patient who is being treated for secondary prevention and provides information to support the management and optimisation of their treatment.
Additional pages are provided for FH Screening, where you can calculate the DCLN score and refer the patient for a FH assessment if required; Hyperlipidaemia Aetiology and LLT’s, containing information on potencies, cautions and medication suitability (adverse reactions, contraindicated, not tolerated).
Get in touch:
If you have any questions regarding access, or the use of the CDRC’s Resources, please get in touch: contact-CDRC@ahsn-nenc.org.uk