The Recall Recovery system was designed in light of the 2020 Covid-19 pandemic but could be used for any situation where LTC reviews have become backlogged. (There is also a linked system for recovery for drugs which require monitoring Drug Requiring Monitoring System)
The system is designed for use by practices using three principle recall systems:
- The CDRC integrated LTC recall system
- A system relying on recording of review SNOMED codes for individual disease e.g. diabetes annual review
- Systems using disease specific recalls
For each system a series of reports are available. (CDRC > Recall Setup > Recall Recovery ……….)
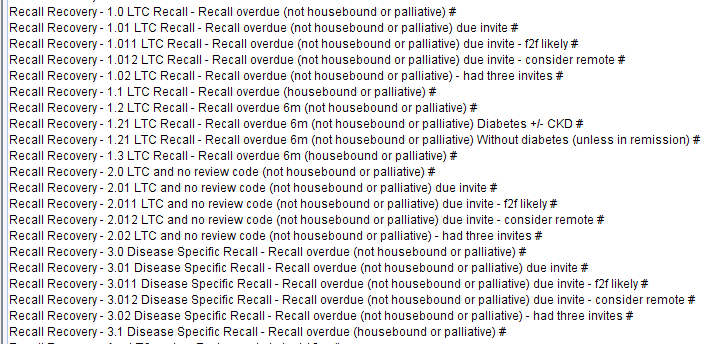
- x.0 – Patients whose review is overdue (excluding those who are housebound or on the palliative care list)
- x.01 – As above who haven’t had an invite in the last month (this report identifies people to be invited at monthly intervals for three months)
- x.011 – Patients in x.01 who are likely to need face to face appointment (see below)
- x.012 – Patients in x.01 who might be able to have a telephone or video review
- x.02 – Patients who have not responded after three invitations
- x.1 – Patients whose review is overdue who are housebound or on the palliative care list
The first four reports can be broken down to show additional details such as those who are shielded, date of recall, patients who are high priority for review (see Appendix 2 – Higher Risk Patients below). Details of how to use the breakdown options are shown below.
For practices using the CDRC LTC system there are also reports to identify those patients overdue a six month review (1.2-1.3) subdivided into those with diabetes (+/-CKD) and those with CKD requiring 6 monthly assessment (without diabetes).
There are also disease specific sets of reports for QoF conditions in the disease specific folders if you wish to concentrate on one disease only e.g. CDRC Quality > Cardiac
Coding Invitations
It is strongly recommended that you use the following code when inviting patients for LTC reviews:
Quality and Outcomes Framework quality indicator-related care invitation (procedure) Y1f8f
This code is used by the system to count who has been invited and how many times. It has the additional advantage of removing patients from the QoF denominator once patients have been invited twice, which will improve end of year QoF performance. NB although the patient is removed from the QoF denominator, TPP have set up new icons that continue to alert the user to QoF issues unlike other QoF exceptions.
Conditions Covered
- For the CDRC LTC Recall system any patients with the LTC Recall will be included
- For the system looking for review codes the following conditions are covered: Asthma, atrial fibrillation, CHD, CKD, COPD, dementia, diabetes, epilepsy, heart failure, hypertension, hypothyroidism, learning disability, serious mental illness, peripheral arterial disease, rheumatoid arthritis and stroke.
- For the system using disease specific recalls the relevant recalls that ‘count’ are shown in Appendix 1 – Disease Specific Recalls, see below. Additional recalls could be added if needed.
Using the Breakdown Option
Right click on the search and choose Breakdown then tick the following options as required. Then click Refresh
| Report | Breakdown Option | Purpose |
| Demographics | First name, surname etc | |
| Recall Recovery * – QoF Invite 1/2/3 (last 6m) # | Event details – event date | Shows the date of recent LTC review invites |
| Recall Recovery * – Higher risk patients # | Strategic reporting ID – Patient ID | Shows patients at higher risk who might be prioritised for review |
| Recall Recovery * – Shielded # | Strategic reporting ID – Patient ID | On the Covid-19 shielding register |
| Has future appointment | Appointment date, clinician etc. | Allows you to see if the patient already has an appointment |
| CDRC LTC Recall System Only (reports 1.x) | ||
| Recall Recovery * – LTC Recall – Recall Overdue # | Recalls – Recall date | Allows you to order the patients by how overdue their review is |
| Disease Specific Recall System Only (reports 3.x) | ||
| Recall Recovery * – Disease Specific Recall – Recall overdue # | Recalls – Recall type and Recall date | Allows you to order the patients by how overdue their review is |
Face to Face vs Remote Reviews
The following conditions are assumed to require at least some face to face assessment (to carry out blood tests or physical examination): Atrial fibrillation, CHD, CKD, diabetes, heart failure, hypertension, hypothyroidism, learning disability, serious mental illness, peripheral arterial disease and stroke.
If patients have the following conditions they are also included in the group likely to need face to face contact: NAFLD, high risk of diabetes, familial hypercholesterolaemia. (NB in systems 2 and 3 these conditions are not specifically included in the reports of patients to recall but do affect location of review. e.g. if a patient has NAFLD only, they will not be included in any of the reports. If a patient has asthma and NAFLD they will be included in the reports but with a recommendation for face to face review).
The following conditions are generally more suited to remote review: Asthma, COPD, dementia, epilepsy, rheumatoid arthritis
Appendices
Appendix 1 – Disease Specific Recalls
Disease specific recalls that are counted in the recall recovery system:
- Asthma
- Asthma annual review
- Atrial fibrillation
- Atrial Fibrillation Annual Review
- CHD
- CHD Annual Review
- CHD Monitoring
- CHRONIC DISEASE MANAGEMENT
- Chronic Disease Monitoring
- Chronic Disease Review
- Chronic Disease Review 12m
- Chronic Disease Review 3m
- Chronic Disease Review 6m
- CKD
- COPD
- COPD ANNUAL REVIEW
- Coronary Heart Disease annual review
- DEMENTIA
- Dementia Annual Review
- Dementia Review
- Diabetes
- Diabetes 3month Review
- Diabetes 6 month check
- Diabetes 6 month review
- Diabetes 6month review
- Diabetes Annual Review
- DIABETES MELLITUS
- Diabetic 6 month review
- Diabetic Annual Review
- Epilepsy
- Heart Failure
- Heart Failure Annual Review
- Hypertension
- HYPERTENSION ANNUAL REVIEW
- Hypertension Monitoring
- Hypothyroidism
- hypothyroidism annual review
- Learning Disabilities
- PVD Monitoring
- Rheumatoid Annual Review
- Rheumatoid Arthritis
- Rheumatoid Arthritis Annual Review
- Rheumatoid Arthritis Monitoring
- Stroke
Appendix 2 – Higher Risk Patients
| Higher Risk | |
| Any LTC | >=4 DNAs in the past 2 years Significantly overdue drug monitoring |
| Asthma | >6 SABA in last 12 months Last ACT score >20 LABA on repeat and no ICS High dose ICS LAMA Aminophylline Biologics Likely moderately severe asthma Exacerbations (>2 in 12, severe/admission last 12m, life threatening) Exacerbation in last 2y but no ICS Concordance issue – LABA, LAMA Exceeding usual quantities of long acting inhalers |
| AF | Anticoagulation should be considered |
| CHD | BP > 150/90 Poor concordance (anticoagulants, antiplatelets, betablocker, ccb, diuretics, RAS drugs, statin) |
| CKD | CKD G3aA3, G3bA2,3, G4/5 |
| COPD | Severe COPD MRC 4+5 >=3 exacerbations in the last year >=3 course of prednisolone in the last year CAT score >20 Concordance issues with long term inhalers |
| Diabetes | Scoring system (1 point for each of) Hba1c>100 Hba1c >75 Hba1c >58 BP >=150/90 High risk feet Mod risk feet ACR >3 ACR>30 Lipid Total Cholesterol>5 Poor concordance hypoglycaemics Poor concordance lipid lowering Poor concordance RAS drugs Poor concordance diuretics Poor concordance CCBs Score >=3 |
| Heart failure | NYHA 3 and 4 Sicubatril Eplerenone, spironolactone |
| Hypertension | BP>=150/90 Poor concordance beta blockers Poor concordance alpha blockers Poor concordance lipid lowering Poor concordance RAS drugs Poor concordance diuretics Poor concordance CCBs |
| Learning disability | BMI <19 or >40 On antidepressants, antipsychotics, anxiolytics, hypnotics, opioids, gabapentinoids, lithium Two or more (non LD) LTCs No health check for 2 years History of aspiration pneumonia or PEG Any drug monitoring is significantly overdue |
| PAD | BP > 150/90 Poor concordance (anticoagulants, antiplatelets, betablocker, ccb, diuretics, RAS drugs, statin) |
| Stroke | BP > 150/90 Poor concordance (anticoagulants, antiplatelets, betablocker, ccb, diuretics, RAS drugs, statin) |