Resources available to support the detection, intervention and management of Hypertension and Blood Pressure.
Accessing CDRC resources on SystmOne
To access the below resources you will need to be a member of the DCS group on SystmOne. To do this, please follow the instructions on the CDRC SystmOne Access webpage.
Reports
CDRC’s Quality Improvement Reports aid to identify patients with possible or un-coded Hypertension and will also help target patients for intervention.
CDRC’s Performance Reports allow you to assess the blood pressure performance of your unit.
Quality Improvement Reports
The following reports are located in the folder CDRC Quality > Cardiovascular and have been categorised into manageable sections; Screening, Casefinding and Management.
Screening
These reports identify patients not currently on the Hypertension register, whose last blood pressure was high. Different blood pressure (BP) thresholds are set to enable the prioritisation of assessment.
These reports are in the folder CDRC Quality > Cardiovascular
- ? Hypertension/BP 1.1 Screening Priority 1 – Consider repeat BP Last BP >=170/105 #
- ? Hypertension/BP 1.2 Screening Priority 2 – Consider repeat BP Last BP >=160/100 #
- ? Hypertension/BP 1.3 Screening Priority 3 – Consider repeat BP Last BP >=150/90 #
- ? Hypertension/BP 1.4 Screening Priority 4 – Consider repeat BP Last BP >=140/90 #
- ? Hypertension/BP 1.5 Screening – Other Groups 1.1 BAME – Consider repeat BP Last BP >=140/90
- ? Hypertension/BP 1.5 Screening – Other Groups 1.2 Core20Plus5 – Consider repeat BP Last BP >=140/90
- ? Hypertension/BP 1.5 Screening – Other Groups 1.3 Hard to reach – Consider repeat BP Last BP >=140/90
- ? Hypertension/BP 1.5 Screening – Other Groups 1.4 Hardest to reach – Consider repeat BP Last BP >=140/90
If your unit has opted into the optional Hypertension Resources or Cardiovascular Resources (see ‘Hypertension Opt-in Resources’ below), these patients will be flagged with the raised BP icon.
Consider inviting these patients for a follow up blood pressure or home blood pressure testing. Patients can be invited systematically using the searches or opportunistically using the patient status alert flag.
It might also be possible to direct them to local pharmacies taking part in the hypertension finding scheme.
Casefinding
The following reports will help identify patients that may not have been appropriately coded.
| Report Name | Returns | Action |
| ? Hypertension/BP 2.1 Casefinding – Potential Hypertension indicator but no HT code | Patients with a code to suggest hypertension (e.g. hypertension annual review) without a QoF hypertension code | The QoF and Contracting template will help to identify the codes (see example below) |
| ? Hypertension/BP 2.2 Casefinding – Medication that might be for HT but no HT | Patients taking medication which might be for hypertension who don’t have an obvious indication for this. | |
| ? Hypertension/BP 2.3 Casefinding – ABPM>=135/85 and not appropriately coded | Patients with a home BP average reading >=135/85 (which defines hypertension) without a subsequent hypertension code. | |
| ? Drug to Diagnosis 004 – Betablocker without obvious indication | Also likely to detect other diagnoses such as hypertension, heart failure, SVT, CHD | |
| ? Drug to Diagnosis 005 – Calcium channel blocker without obvious indication | Also likely to detect other diagnoses such as hypertension, Raynauds, SVT, CHD | |
| ? Drug to Diagnosis 007 – RAS Drug without obvious indication | Also likely to detect other diagnoses such as CHD, diabetic kidney disease, heart failure, LVSD | |
| ? Drug to Diagnosis 009 – Thiazides without obvious indication |
Management
The following reports will help target patients for intervention. They have been arranged in such a way to facilitate prioritisation.
| Report Name | Returns | Intervention | Notes |
| ? Hypertension/BP 3.1 Management Priority 1 – Highest potential for intervention | Priority 1 patients. Has all three of: – 3 months overdue BP check. – Suspected poor concordance. – BP is >20/10 over NICE or personal target. | Review patient | |
| ? Hypertension/BP 3.2 Management Priority 2 – High potential for intervention | Priority 2 patients. Has two out of three of: – 3 months overdue BP check. – Suspected poor concordance. – BP is >20/10 over NICE or personal target. | Review patient | Patients with stage 1 hypertension without end organ damage who are off treatment are not included. Patients are not included if the last blood pressure was recorded in the last 6w allowing time for recent intervention to have an effect |
| ? Hypertension/BP 3.31 Management Priority 3a – Consider treatment intensification | Priority 3a Last BP is >30/15 above NICE or personal target. | Review patient and consider treatment intensification | Patients in priority 1 and 2 are excluded. |
| ? Hypertension/BP 3.32 Management Priority 3b – Consider Poor Concordance | Priority 3b Patients who need BP control who do not appear to be collecting antihypertensives | Consider review of concordance | Patients in priority 1 and 2 are excluded. |
| ? Hypertension/BP 3.33 Management Priority 3c – No BP check for 18m | Priority 3c Patients who need a BP check who are at least 6 months overdue | Consider inviting for review or requesting home BP | Patients in priority 1 and 2 are excluded. This includes patients with AAA, CHD, CKD, diabetes, hypertension, heart failure, PAD, stroke/TIA. |
| ? Hypertension/BP 3.41 Management Priority 4a – Consider treatment intensification | Priority 4a Last BP is >20/10 above NICE or personal target | Review patient and consider treatment intensification | Patients in priority 1 and 2 are excluded. |
| ? Hypertension/BP 3.43 Management Priority 4c – No BP check for 15m | Priority 4c Patients who need a BP check who are at least 3 months overdue a check | Consider inviting for review or requesting home BP | Patients in priority 1 and 2 are excluded. This includes patients with AAA, CHD, CKD, diabetes, hypertension, heart failure, PAD, stroke/TIA. |
| ? Hypertension/BP 3.5 Management Priority 5 – Consider treatment intensification | Priority 5 Last BP is above NICE or personal target | Review patient and consider treatment intensification | Patients in priority 1 and 2 are excluded. |
| ? Hypertension/BP 3.6 Management Priority 6 – Consider setting personal target | Priority 6 Patients who need BP control who don’t have a personal target | Consider setting a BP target | Includes: – Hypertension (unless stage 1 without end organ damage – Type 1 diabetes – Diabetes with micro/albuminuria – CKD |
Performance Reports
The following reports allow units to assess their performance with respect to blood pressure management. These searches cover people with any condition for which BP control is recommended – CKD, Diabetes, Hypertension and Stroke/TIA
Templates
BP Detailed Blood Pressure
How to Access
In the lower left hand corner use the search bar, type in ‘BP Detailed Blood Pressure’ and select the following template:

Alternatively, press F12 and search for ‘BP Detailed Blood Pressure’, this will return the aforementioned template.
Blood pressure can be recorded on the Core Data Entry template or more detailed blood pressure information can be seen/recorded on the BP Detailed Blood Pressure template which be reached from the Core Data Entry template or added to existing toolbars or templates.
The BP Detailed Blood Pressure template has the following features
| Column 1 | Column 2 | Column 3 |
| Space to record specific requirements for BP recording e.g. cuff size, which are to use/avoid | Most recent blood pressure monitoring comments | |
| Link to BP Targets setting template | Current estimated NICE BP target Current QoF target Current patient specific target (if this has been set) | Indicator to describe current QoF performance regarding blood pressure (all QoF domains) |
| Link to BP Exceptions template | ||
| Space to record various clinic BPs | Most recent BP readings (all types) | Link to BP Graph which shows more detailed information about previous BP reading in data or graphical form |
| Relevant home blood pressure codes Link to a printable home BP record sheet Link to the Communication Annexe to send SMS or email links for a BP recording sheet. Link to an average calculator Space to record home or ambulatory BP | Relevant information about previous home and ambulatory BP readings and codes |
The Guidance page has information about recording blood pressure and diagnosing hypertension
The Resources page has links to professional resources and a button to link to patient resources
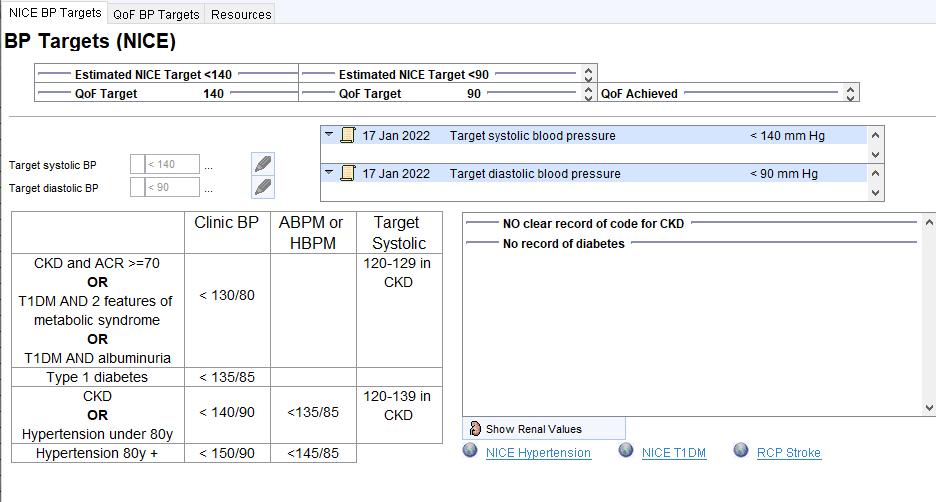
Blood Pressure Target Setting
How to Access
In the lower left hand corner use the search bar, type in ‘BP Targets’ and select the following template:

Alternatively, press F12 and search for ‘BP Targets’, this will return the aforementioned template.
The BP Target template shows estimated targets (NICE and QoF as these are not always aligned) and allows recording of patient specific targets. If a target is set which is not the default, it is helpful to record this as free text with the target – this free text will be displayed in the panel on the right.
Blood Pressure Treatment
How to Access
In the lower left hand corner use the search bar, type in ‘BP Treatment CDRC’ and select the following template:

Alternatively, press F12 and search for ‘BP Treatment’, this will return the aforementioned template.
The BP Treatment template provides guidance about how to treat blood pressure. The home page sets out BP targets, current treatment and the NICE pathway.
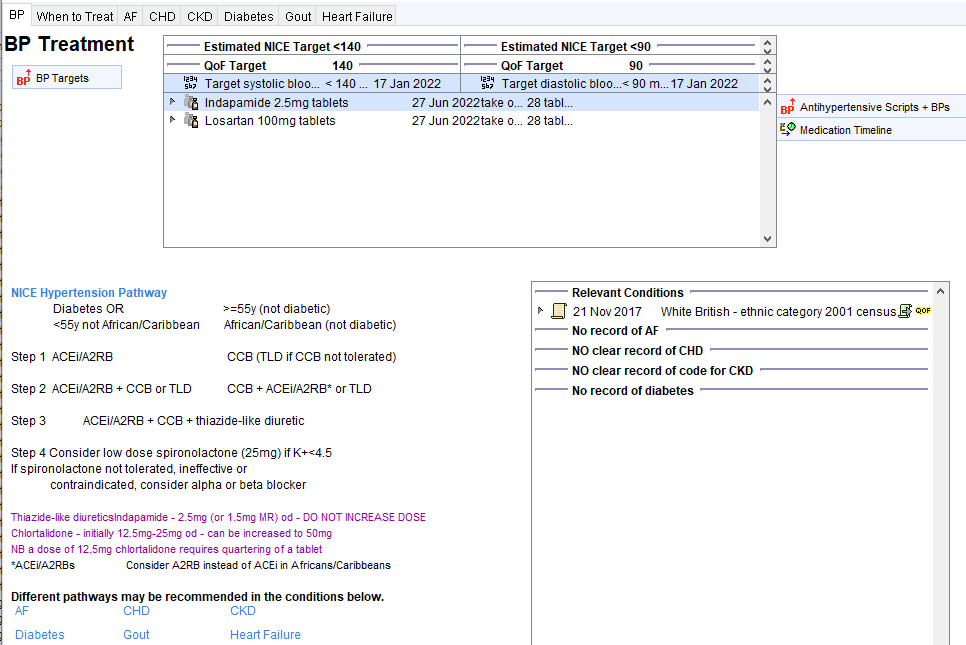
The When to Treat Page, provides guidance on when to start treatment.
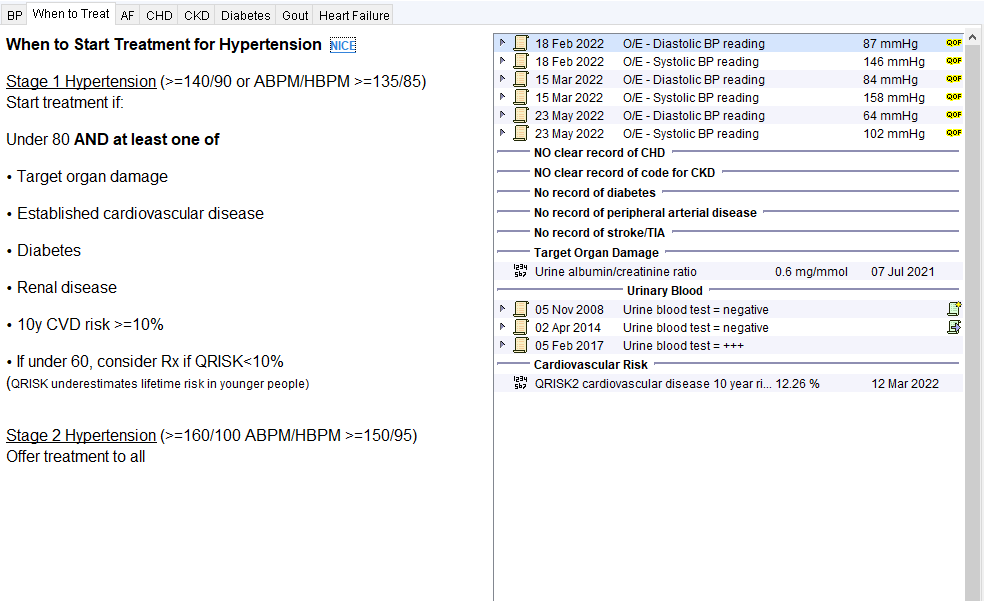
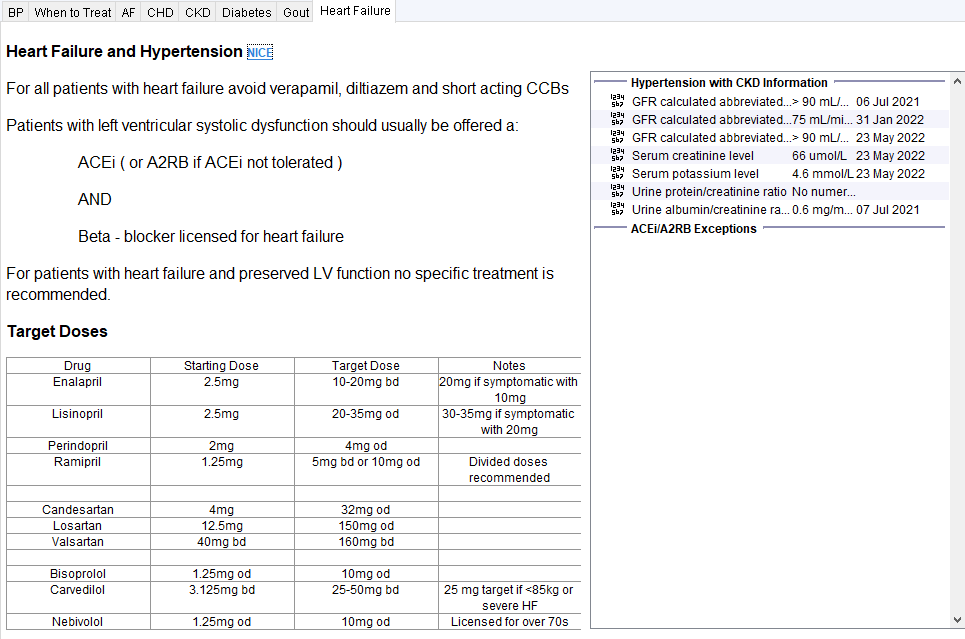
There is also Disease specific pages which hosts guidance.
Hypertension CDRC Template
How to Access
In the lower left hand corner use the search bar, type in ‘Hypertension CDRC’ and select the following template:

Alternatively, press F12 and search for ‘Hypertension CDRC’, this will return the aforementioned template.
The Hypertension CDRC template facilitates the review of patients with hypertension.
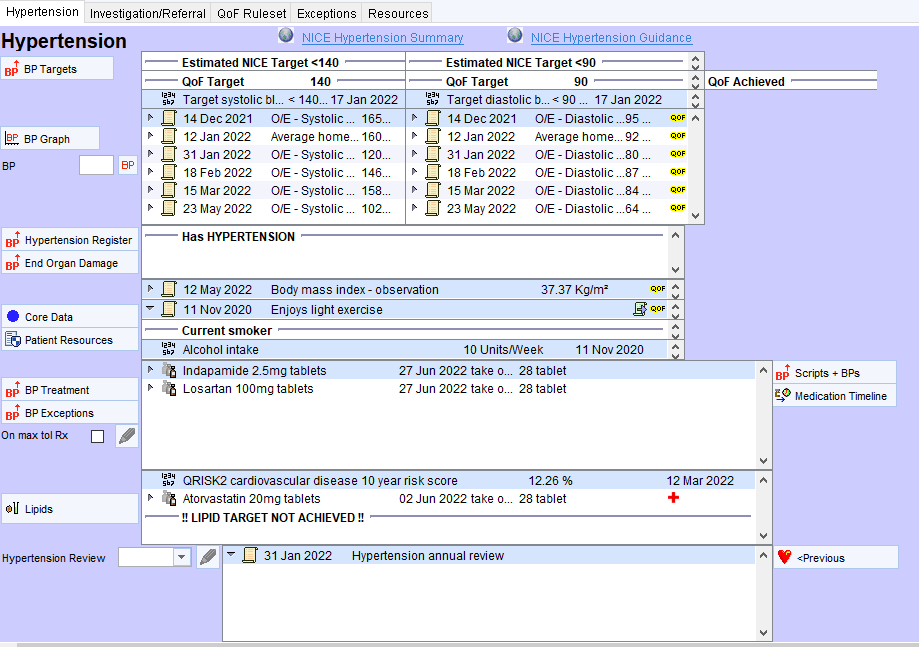
The Hypertension CDRC template features:
- Information about estimated and actual BP targets with a link to the BP Target Setting template to record/update BP targets. QoF achievement is shown (this covers achievement for all BP related QoF indicators not just the hypertension domain).
- Recent blood pressure readings (of any type) and a link to the BP graph function.
- A panel which shows if the patient is on the hypertension register and specifically shows if the patient has stage 1 hypertension without end organ damage. Information about end organ damage is shown here. There are links to templates to add/remove patients from the hypertension register and to view and record information about End Organ Damage.
- A panel showing key lifestyle factors which contribute to hypertension. There is a link to the Core Data template to record lifestyle factors and deliver interventions / referrals. There is a link to patient information to manage blood pressure
The BP treatment panel shows current antihypertensive medication and will show prompts when applicable such as:
- Consider setting BP target
- Consider intensification of treatment
- Consider ACEi/A2RB when this is specifically indicated e.g. diabetic kidney disease
- Consider drug concordance when patients are not collecting antihypertensives.
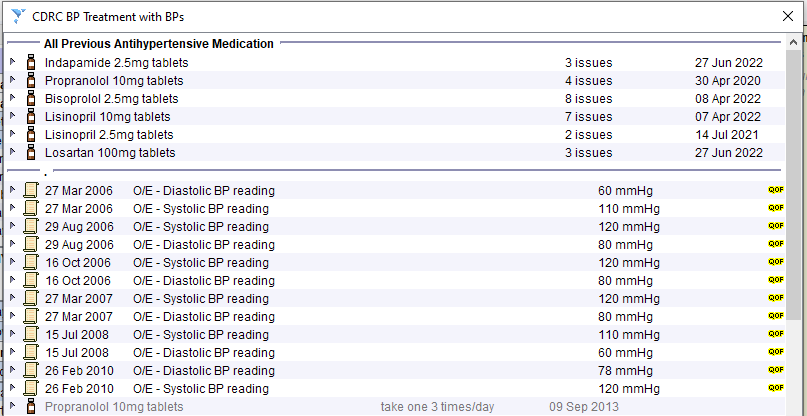
There is a link to the BP Treatment template which shows the NICE pathway for treating raised blood pressure. There is also a link to record hypertension exception codes. The Scripts and BPs button will show previous antihypertensives along with BP readings making it easier to review progress with current and previous treatment.
There is a panel showing information and CVD risk and lipid lowering therapy with a link to the lipid template
There is space to record that the review has been completed along with any relevant comments. The most recent review (and any comments) are shown in the panel alongside.
Hypertension End Organ Damage
How to Access
In the lower left hand corner use the search bar, type in ‘Hypertension End Organ Damage’ and select the following template:

Alternatively, press F12 and search for ‘Hypertension End Organ Damage’, this will return the aforementioned template.
The Hypertension End Organ Damage template shows relevant information.
Previous information about renal function/proteinuria/haematuria can be displayed by clicking the <Expand button
The last ECG can be viewed by right clicking on it and choosing View content.
![Hypertension End Organ Damage
Conditions suggesting end organ damage include:
CHO
Heal failure
Left ventricular hypertrophy
Stroke
Kidney Damage
Assess renal function
Assess renal protein loss
Urine blood
Eye Damage
Fundoscopy
ECG Changes
12 lead ECG
No record of AF
NO clear record of CHO
NO clear record of code for CKD
No record of heart failure
No record of peripheral arterial disease
No record of strokefflA
23 May 2022
23 May 2022
07 Jul 2021
07 Jul 2021
02 Apr 2014
5 Feb 2017
Serum creatinine level
GFR calculated abbreviated MDRD
Urine albumin/creatinine ratio
Urine albumin/creatinine ratio
Urine blood test = negative
Urine blood test
66 umol/L
> go mUminm
0.6 mgJmmol
<Expand
CDRC Fundoscopy (last) view has no data for patient
C]
16 Nov 2007
06 Jul 2021
06 Jul 2021
ECG normal
ECG to Leadgate Surgery
121eadECG](https://cdrc.nhs.uk/wp-content/uploads/2022/10/image-43.png)
Additional Resources
Hypertension and Blood Pressure Patient Information Leaflet
This Patient Information template has links to useful patient resources – both weblinks and some printable resources for use from face to face consultations.
There is a link to the Communication Annexe which makes it easy to send information electronically to patients. This also allows the patient to send completed BP sheets back to the practice.
Hypertension Opt-in Resources
For practices who have recently joined the DCS group on SystmOne, PSAs and Protocols will not be automatically active. You can choose the level of activation you would like; opt-in to all or resource specific CDRC resource PSAs and Protocols. Alternatively you can choose not to opt-in and only use the Reports and Templates.
If you would like to activate that following, or all, CDRC PSAs and Protocols, please email contact-cdrc@ahsn-nenc.org.uk
The following resources are available to support Hypertension, Blood Pressure management and QoF Performance:
| Resource | Trigger | Action |
| Raised BP PSA (icon) | Displays for patients not on the hypertension register with raised BP | Consider repeat BP or home BP |
| BP Target Protocol | Will trigger if the patient’s estimated BP target changes e.g. at new hypertension diagnosis | Consider adding a BP target |
Supporting Blood Pressure at Home
The following resources are available to support Blood Pressure at home.
Reports
The following searches will help identify patients who might benefit from blood pressure measurements at home.
These reports are found in the folder CDRC Quality > Cardiovascular
Report 1.10 identifies patients who need BP management (hypertension, diabetes, CKD) who have not achieved the NICE target for their combination of risk factors, unless they have a target BP recorded that has been achieved. People with moderate or severe frailty, care home residents and palliative care stages B/C/D are excluded.
Report 1.11 identifies patients in 1.10 who have had a record (in the past 12 months) of home BP measurement, referral for home BP, home BP not indicated, home BP declined.
The other searches use the same criteria but identify patients at increasing levels of risk, based on factors such as last BP level, comorbidities, history of engagement, concordance.
Template
Use the BP Detailed Blood Pressure template, highlighted above, to record relevant information and values
Use the PIL Hypertension and Blood Pressure template below for providing patient information.