TPP have recently changed the codes in the learning disability code cluster. This is usually done at the request of NHSE. There is a sizeable list of new codes on the list which appears to have increased practices’ LD Register by approximately 15%. The LD DES numbers are also affected.
From an initial audit, many of these patients do not have a learning disability. The ‘new patients with learning disability’ can be categorised into four groups:
- Patient who do have a learning disability which had not been given a previous LD code.
- Patients with coding errors – patients who have incorrectly been given a code indicating a learning disability. The commonest examples of this appear to be:
- Coded with Sjogren-Larsson syndrome (which is associated with LD) rather than the much commoner Sjogren’s syndrome (which is not).
- Coded with Dysequilibrium syndrome (which is a very rare condition associated with LD) during a consultation for dizziness.
- Patient with conditions which are unlikely to be associated with LD. The commonest example of this is retinitis pigmentosa. Although there are some very rare syndromes or RP associated with a wider spectrum of problems including LD, the majority of people with RP do not have a learning disability.
- Patients with conditions which are associated with learning disability in only a proportion of affected patients, i.e. many patients with these conditions do not have a learning disability. The commonest examples of this category are Fragile X syndrome (especially females who can have a very mild form of the disease), fetal alcohol syndrome, neurofibromatosis type 1 and phenylketonuria (where treated patients are very unlikely to have a learning disability). A list of some of the commoner codes which have been added to the learning disability cluster are attached to the bottom of this email.
This change is likely to have adverse outcomes for patients, practices and the NHS. These will include:
- Patients being inappropriately invited for LD health checks.
- Additional practice administration and clinical time dealing with the erroneous inclusions on the LD register.
- Patient distress at being told they have a learning disability.
- Inappropriate exclusion from some referral pathways where significant learning disability is an exclusion criteria.
- Inappropriate exclusion from some clinical trials (where LD is an exclusion criteria).
- An overestimate of the numbers of patients with LD on GP registers.
- Potential impacts for patients trying to access certain occupational or educational opportunities, where a learning disability might be a barrier.
The following CDRC resources are available to help maintain the accuracy of your LD Registers in the light of recent changes made by NHSE.
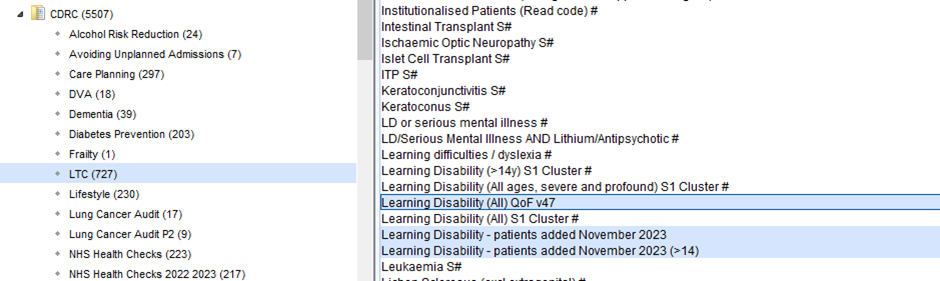
The following searches show your LD register population before and after the introduction of the new codes:
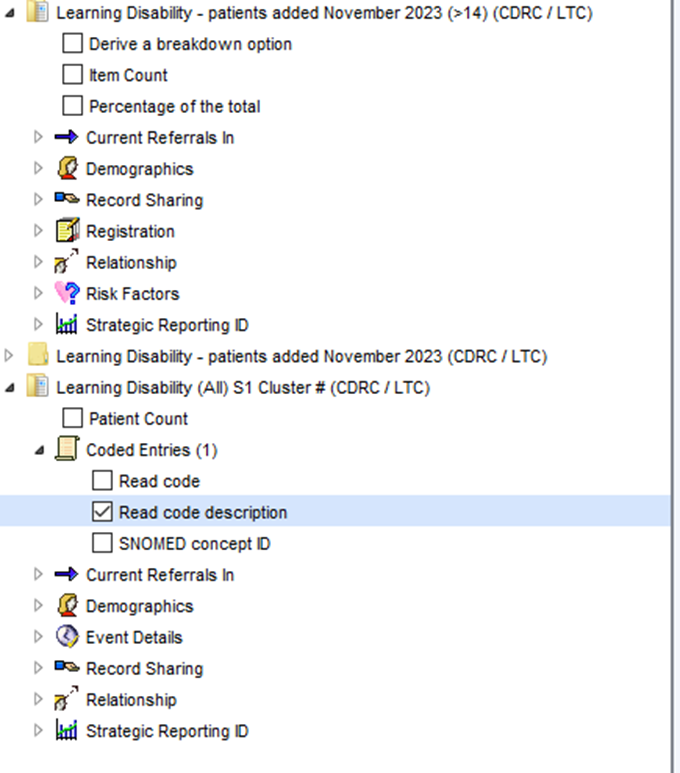
To see the implicated codes for all patients use the breakdown option, selecting this breakdown (along with any demographics you need):
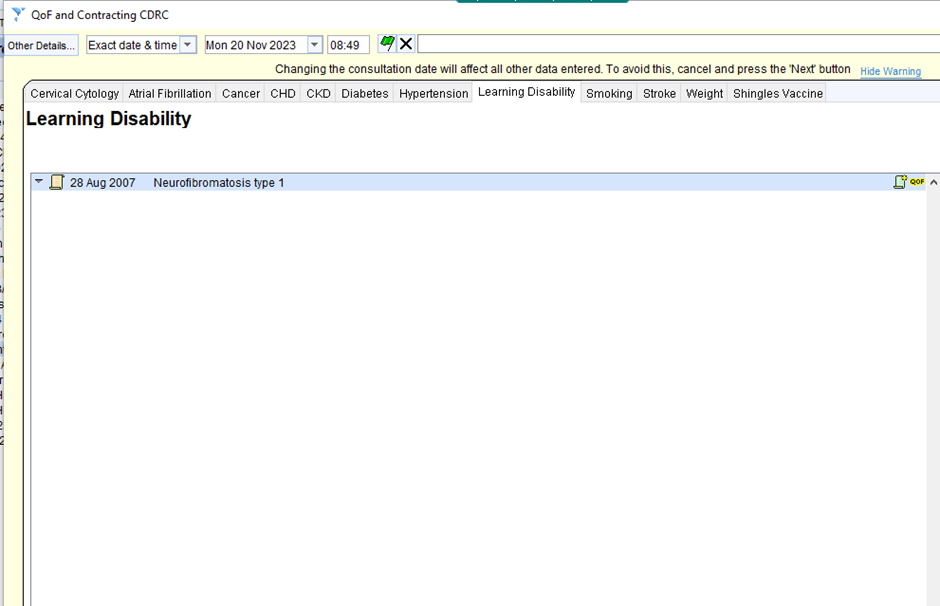
For individual patients the QoF and Contracting template (accessed via Template Master CDRC) will show you the relevant codes:
Commoner codes added to the learning disability cluster:
| (Macroencephaly)(megalencephaly)(enlarg brain)(macrocephaly) |
| (Marinesco-Sjogren syndrome) or (disorder of metabolism NOS) |
| Alpha-D-mannosidosis |
| Benign myoclonic epilepsy in infancy |
| Carpenter’s syndrome |
| Craniodiaphyseal dysplasia |
| Dysequilibrium syndrome |
| Fetal alcohol syndrome |
| Fragile X syndrome |
| Hydrocephalus with anomaly of aqueduct of Sylvius |
| Klinefelter’s syndrome, XXYY |
| Lennox-Gastaut syndrome |
| Marinesco-Sjogren syndrome |
| Megalencephaly |
| Neurofibromatosis type 1 |
| Pallister-Killian syndrome |
| Phenylketonuria |
| Primary microcephaly |
| Retinitis pigmentosa |
| Sjogren-Larsson’s syndrome |
| Thanatophoric dwarfism |
| Weaver syndrome |
| William syndrome |
| Wilson’s disease |
| X-linked adrenoleucodystrophy |
| Xeroderma pigmentosum |